
Joint Commission Workplace Violence Prevention Requirements (2026): What Hospitals Should Know

Healthcare workers face violence more than any other profession.
Yes, that’s not an exaggeration. Nearly 75% of all workplace violence incidents occur in healthcare settings, and many cases never get reported. What used to be considered part of the job is now becoming one of the biggest operational risks hospitals face.
Workplace violence shows up in many forms. It can be a patient becoming aggressive in the ER, a behavioral health escalation, or a visitor reacting under stress. These are not isolated incidents. They happen across departments, across shifts, and often in environments where staff already operate under pressure.
Over time, the impact compounds. Teams experience higher levels of stress, burnout becomes more common, and hospitals struggle to retain experienced staff. When workplace violence becomes frequent, it starts affecting not just the workforce but the overall quality and consistency of patient care.
This is exactly why workplace violence prevention is no longer optional. Regulators are tightening expectations, and the Joint Commission workplace violence 2026 update reflects that shift. Hospitals are now expected to move beyond reactive measures and implement structured, well-documented prevention strategies.
If you are responsible for compliance or operations, this change has direct implications for how your organization assesses risk, trains staff, and responds to incidents as they happen.
In this guide, you will understand the scale of workplace violence, key workplace violence facts, and real workplace violence examples across healthcare settings. You will also get a clear breakdown of TJC workplace violence prevention requirements and what they mean in practice.
The Growing Crisis: Workplace Violence in Healthcare
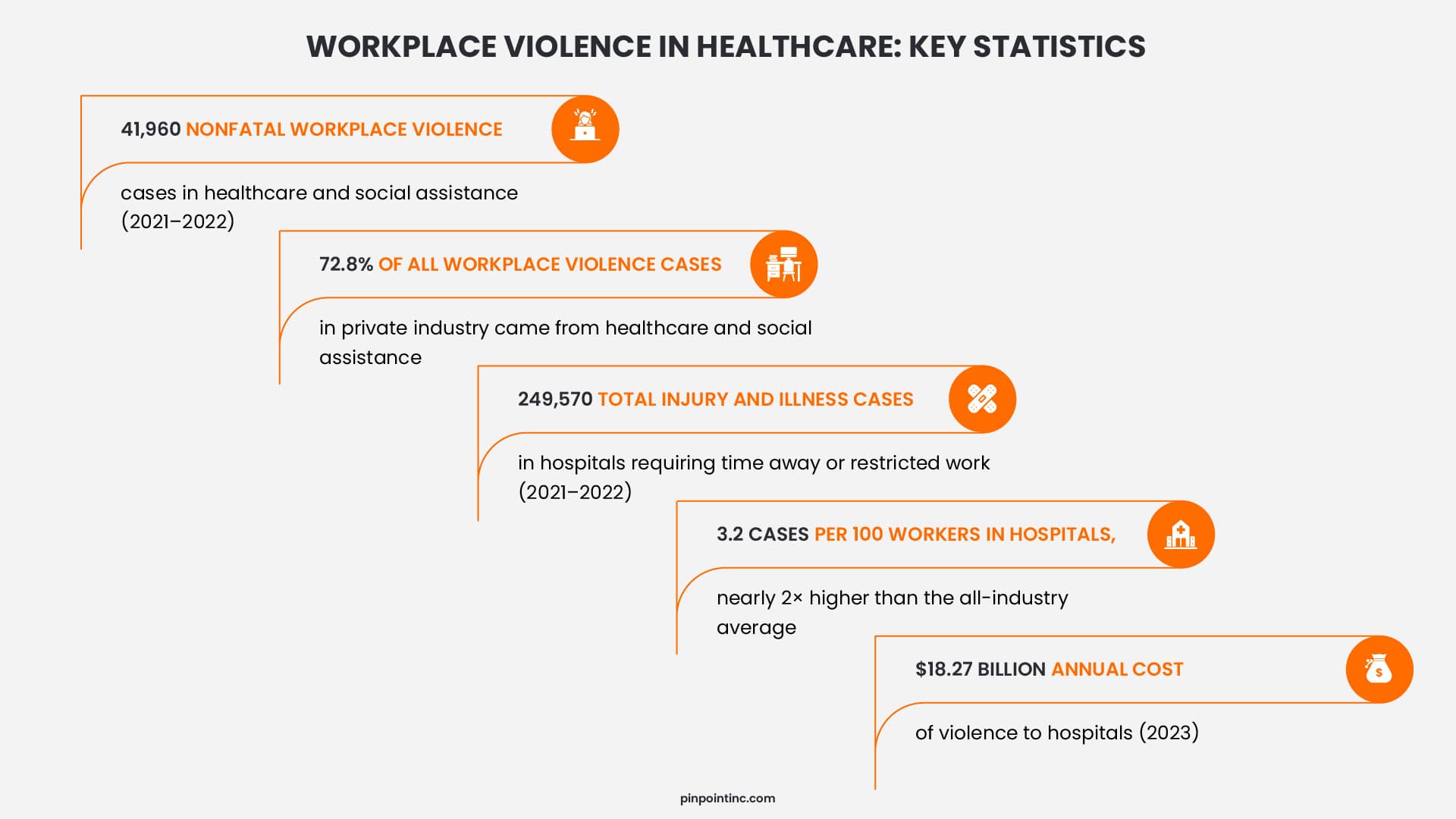
The numbers around workplace violence in healthcare point to a clear pattern rather than isolated incidents. Between 2021 and 2022, healthcare and social assistance reported 41,960 nonfatal workplace violence cases, accounting for 72.8% of all such cases in private industry. This concentration highlights how workplace violence is not evenly distributed across sectors but heavily centered in healthcare environments.
The broader working conditions in hospitals reinforce this risk. OSHA data shows that hospitals recorded 249,570 injury and illness cases requiring time away from work or restricted duties during the same period, with an incidence rate nearly double the all-industry average. While not all of these cases are workplace violence, they reflect the intensity and unpredictability of hospital settings where such incidents are more likely to occur.
Healthcare workers operate in environments shaped by urgency, emotional stress, and high patient acuity. Emergency departments and behavioral health units, in particular, see frequent escalation points where workplace violence can emerge quickly. These conditions, combined with staffing constraints and long wait times, increase both exposure and vulnerability.
When compared to other industries, healthcare stands out not just because of higher numbers but because of the nature of daily interactions. This is why workplace violence prevention is becoming a central focus for hospitals, both from a safety perspective and as part of meeting evolving regulatory expectations.
Workplace Violence Facts Every Hospital Leader Should Know
Workplace violence facts become more meaningful when you look at their direct impact on hospital operations. The American Hospital Association estimates that violence costs hospitals $18.27 billion annually, driven by medical treatment, legal exposure, staff replacement, and increased security requirements.
A large portion of this burden comes from staff turnover, particularly nurses who face repeated exposure to workplace violence. Over time, this leads to burnout, absenteeism, and difficulty retaining experienced staff. This pattern is already visible across healthcare systems where workforce stability is becoming harder to maintain, especially in high-pressure environments.
When you look beyond individual hospitals, workplace violence shows a consistent pattern across regions, which reinforces that this is not an isolated issue.
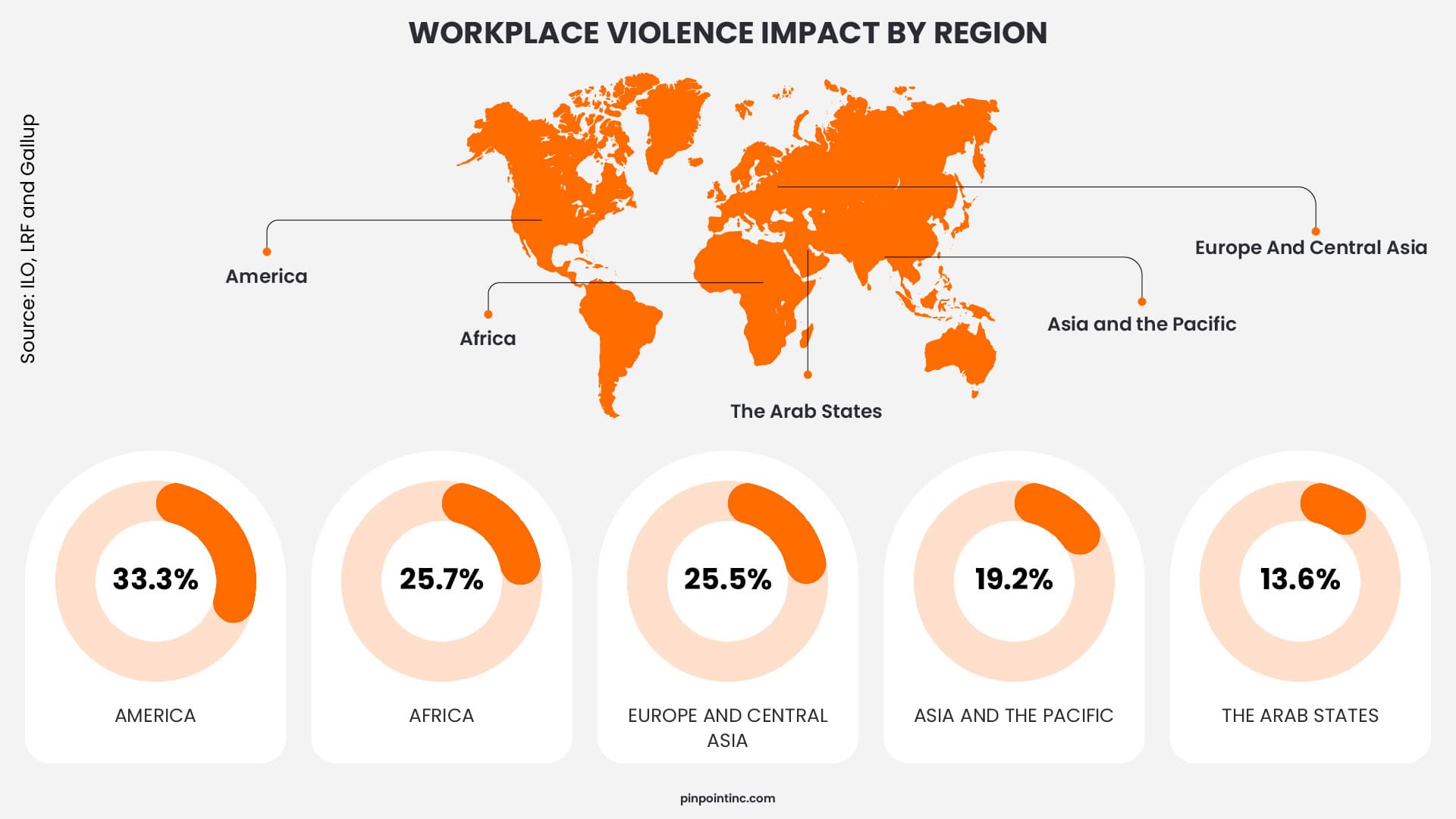
This distribution shows that workplace violence is present across healthcare systems globally, with higher exposure in regions where patient demand and workforce pressure are more intense.
Beyond staffing and cost, workplace violence also affects how care is delivered. The Joint Commission notes that these incidents can reduce staff focus, slow response times, and create environments where both caregivers and patients feel less safe.
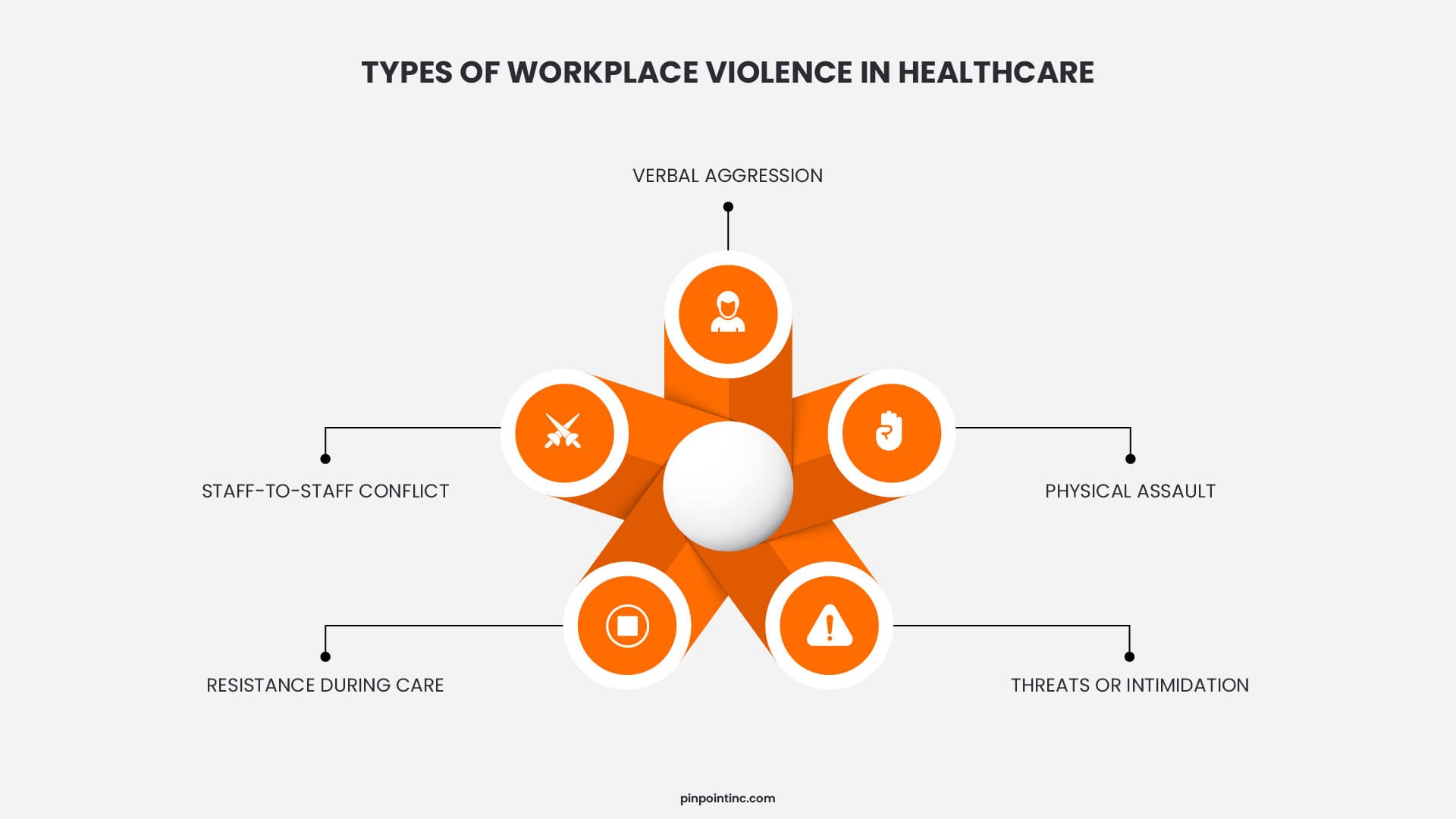
Common Workplace Violence Examples in Healthcare Settings
Workplace violence examples in healthcare tend to follow recurring patterns tied to specific departments and situations. These incidents are not random. They are often linked to pressure points in patient care, communication gaps, and high-stress environments.
Here are the most common workplace violence examples seen across healthcare settings:
Emergency Department (ER)
- Patients reacting aggressively to long wait times
- Visitors becoming confrontational during critical situations
- Escalation from verbal threats to physical aggression
Behavioral Health Units
- Patients experiencing mental health crises or withdrawal
- Physical resistance during intervention or restraint
- Sudden escalation during routine care
Visitor-Driven Incidents
- Family members reacting to unclear communication
- Emotional distress turning into verbal or physical confrontation
- Disputes over treatment decisions or delays
Inpatient and General Care Units
- Frustration during ongoing treatment or recovery
- Conflict during medication administration or care routines
- Repeated low-level aggression that escalates over time
Admissions, Transport, and Discharge
- Patients resisting movement or instructions
- Agitation during intake or discharge processes
- Limited staff presence increasing risk during transitions
Internal Staff Conflict
- Tension from long shifts and workload pressure
- Verbal disputes escalating between colleagues
- Stress-driven interactions affecting team dynamics
Why Workplace Violence Prevention is Now a Regulatory Priority
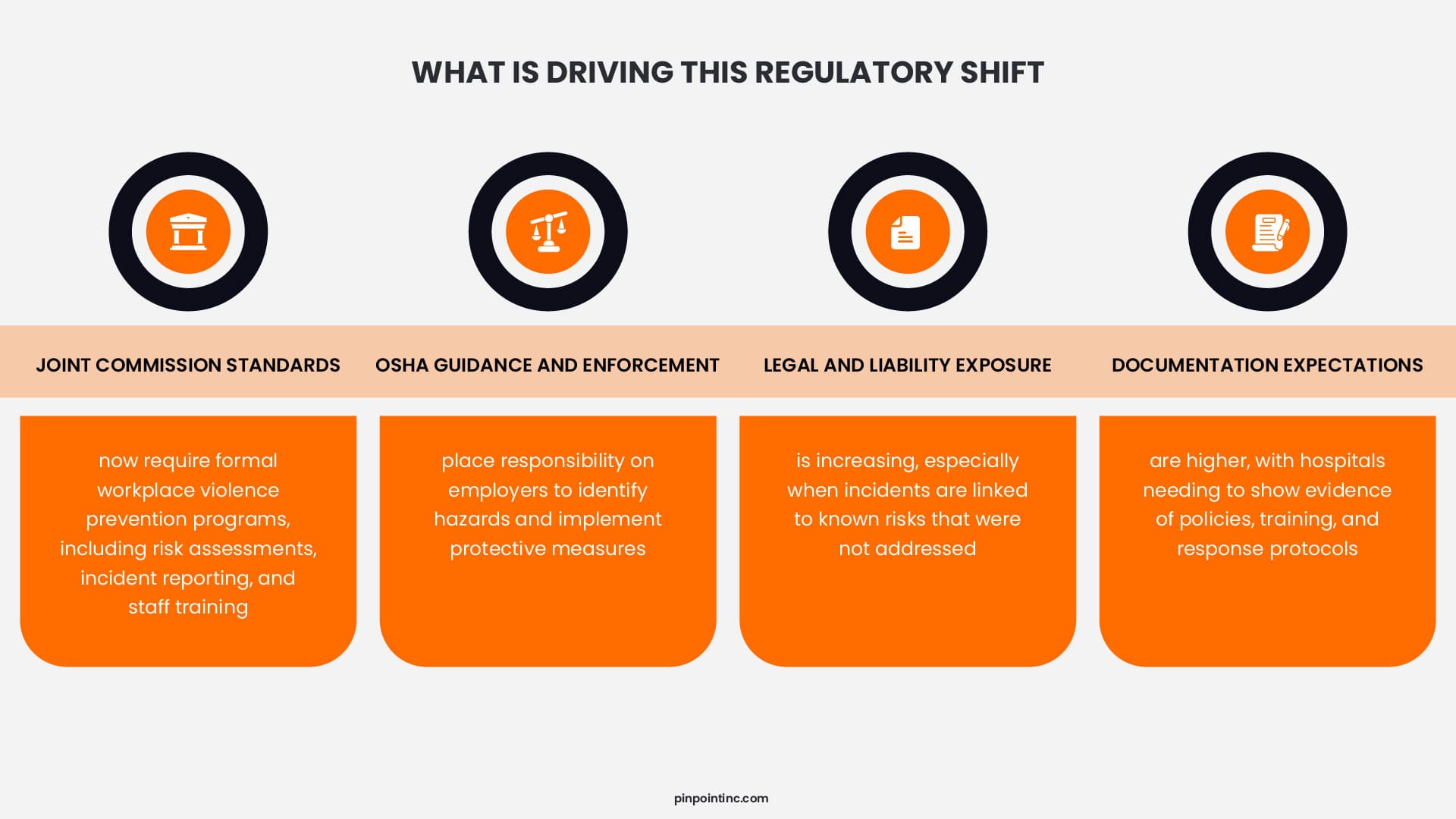
Workplace violence prevention is no longer treated as a secondary safety initiative but has become a regulatory requirement driven by rising incident rates, workforce impact, and increased scrutiny from accrediting bodies. Healthcare organizations are now expected to demonstrate that they have structured systems in place to identify, manage, and reduce workplace violence risks.
This shift is largely shaped by The Joint Commission and OSHA, both of which have moved toward clearer expectations around employer responsibility. Hospitals are no longer assessed only on whether incidents occur, but on whether they have taken proactive steps to prevent them.
The risk of non-compliance goes beyond fines or citations. It can impact accreditation status, increase legal exposure, and weaken workforce stability. This is why workplace violence prevention is now treated as a core operational requirement rather than an optional initiative.
Joint Commission Workplace Violence Prevention Requirements (2026)
When people search for joint commission workplace violence 2026, they are usually trying to understand what hospitals are expected to have in place now. The most useful answer is this: The Joint Commission already established a formal framework for hospital workplace violence prevention, and in 2026 that framework sits within a new accreditation structure that places clearer focus on measurable goals. For hospitals and critical access hospitals, the issue is not whether workplace violence prevention is optional. It is whether the organization can show that its program is active, documented, and consistently implemented.
The Joint Commission’s workplace violence prevention framework centers on leadership oversight, written processes, incident reporting, data review, staff education, and post-incident follow-up. In practice, that means hospitals need more than a policy on paper. They need a working program that leadership reviews, staff understand, and surveyors can trace through training records, event reports, and corrective actions. This is why TJC workplace violence prevention has become a practical compliance issue rather than a general safety discussion.
Key Requirements
- Leadership accountability: Hospital leaders are expected to oversee the workplace violence prevention program and support its implementation across the organization.
- Risk assessments: Hospitals are expected to evaluate where workplace violence risks are most likely to occur and use that information to shape prevention efforts.
- Reporting systems: Staff need a defined way to report incidents, threats, and concerning behavior so the hospital can track patterns and respond appropriately.
- Data collection and analysis: Joint Commission expects organizations to review incident data, identify trends, and use findings to improve the program over time.
- Staff training and education: Training must cover prevention, recognition, response, and reporting, and it is expected at hire, annually, and when program changes occur.
- Incident response and post-incident protocols: Hospitals need processes not only for immediate response, but also for follow-up, investigation, and support after an event.
What’s New in 2026
The biggest 2026 change is structural rather than substantive. Joint Commission’s National Performance Goals chapter became effective for hospitals and critical access hospitals on January 1, 2026, replacing the former National Patient Safety Goals chapter. Joint Commission has said that this new chapter does not introduce new requirements, but it does organize existing requirements into clearer, measurable goals. That means hospitals should expect sharper survey conversations around whether their workplace violence prevention program is visible, documented, and operating as intended.
For hospitals, that raises the bar in three practical ways:
Stronger enforcement visibility – Even without brand-new rules, clearer goal-based organization makes gaps easier to identify during accreditation review.
Documentation expectations – Hospitals need evidence that risk assessments, training, reporting, and follow-up are actually happening, not just described in policy language.
Staff protection expectations – The program must show that the organization is actively preparing staff to prevent, recognize, report, and respond to workplace violence.
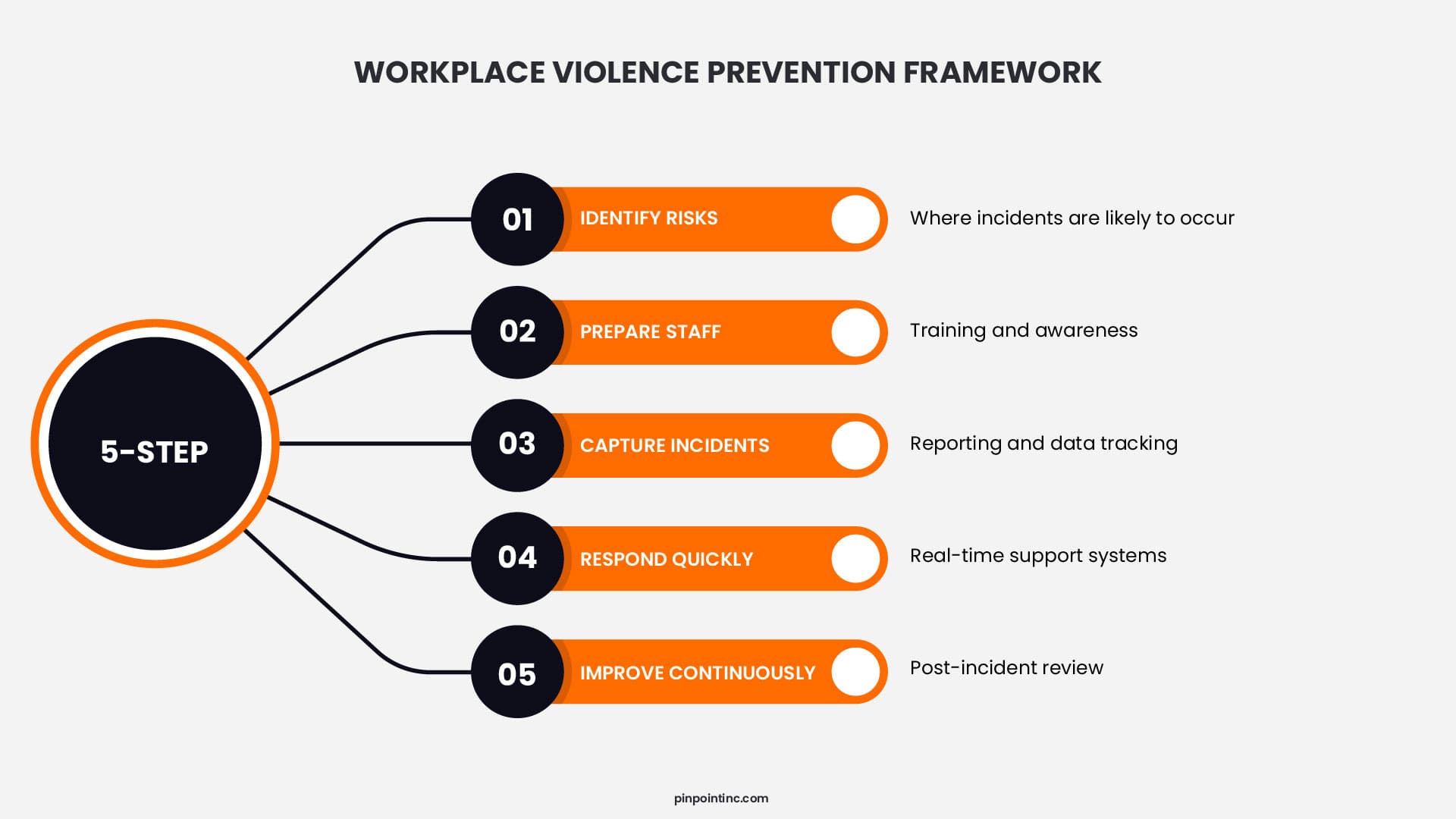
Step-by-Step Workplace Violence Prevention Framework
Workplace violence prevention becomes effective only when it is built into daily operations rather than treated as a policy document. Hospitals that manage this well tend to follow a structured approach where risk identification, staff readiness, and response systems work together.
Instead of viewing prevention as a single initiative, it helps to break it into a repeatable framework that can be implemented across departments.
Step 1: Risk Assessment
Every workplace violence prevention program starts with understanding where and how incidents are most likely to occur. This involves reviewing past incidents, identifying high-risk departments such as emergency or behavioral health, and mapping specific triggers like wait times, patient conditions, or staffing gaps.
Risk assessment should not be a one-time exercise. It needs to be updated regularly as patient volume, staffing, and operational conditions change.
Step 2: Staff Training
Training plays a central role in workplace violence prevention because frontline staff are often the first to recognize early warning signs. Effective programs go beyond basic awareness and focus on practical skills such as de-escalation techniques, recognizing behavioral cues, and knowing when to call for support.
Training also needs to be continuous. New hires, annual refreshers, and scenario-based learning help ensure that staff can respond confidently in real situations.
Step 3: Reporting Systems
A workplace violence prevention program is only as strong as its reporting process. Staff need a clear, simple way to report incidents, threats, or near misses without hesitation. If reporting is complicated or time-consuming, incidents go unrecorded and patterns are missed.
Hospitals that perform well in this area treat reporting as a routine part of operations and use the data to identify trends and recurring risks.
Step 4: Real-Time Response
When an incident occurs, response speed and coordination make a significant difference. Staff need immediate access to support, whether that is security, clinical backup, or communication systems that alert nearby teams.
This is where many workplace violence prevention programs fall short. Having policies is not enough if response tools are slow or unclear. Real-time response should be simple, reliable, and easy to activate under pressure.
Step 5: Post-Incident Review
The final step in workplace violence prevention is often overlooked but critical for long-term improvement. Every incident should be reviewed to understand what happened, how it was handled, and what can be improved.
This includes supporting affected staff, updating protocols if needed, and feeding insights back into training and risk assessment. Without this step, the same issues tend to repeat.
The Role of Technology in Workplace Violence Prevention
Technology has become a key part of workplace violence prevention, especially in environments where incidents can escalate quickly and require immediate coordination. Hospitals are increasingly relying on systems that improve visibility, communication, and response speed across departments.
One of the most widely used tools is real-time alert systems like wearable panic button solutions that allow staff to quickly signal for assistance during an incident. These systems are designed to notify nearby personnel or security teams without disrupting patient care, helping reduce response time when seconds matter.
Communication platforms also play an important role. Integrated tools such as secure messaging systems and centralized dashboards allow teams to share information about potential risks, ongoing incidents, or patient behavior in real time. This improves coordination and ensures that staff are not responding in isolation.
Another layer of workplace violence prevention involves video monitoring and access control systems. Surveillance helps monitor high-risk areas, while controlled access limits unauthorized movement within sensitive zones like emergency departments or behavioral health units.
At the same time, privacy concerns remain an important consideration. Continuous tracking of staff can create discomfort and raise compliance questions, which is why many healthcare organizations are evaluating solutions that support safety without relying on constant location monitoring.
Ultimately, the effectiveness of these technologies depends on how quickly they enable response. In high-risk situations, delays in communication or unclear escalation pathways can increase the severity of incidents, which is why workplace violence prevention strategies continue to prioritize speed, reliability, and ease of use.
Closing
So far, you’ve seen why workplace violence is no longer a secondary concern in healthcare. The scale of incidents, the regulatory pressure, and the impact on staff and patient care all point to the same reality. This is a problem that requires structured, real-time solutions.
As expectations from the Joint Commission continue to evolve, workplace violence prevention will increasingly be measured by how effectively hospitals can respond in the moment and protect their teams during critical situations. Policies and training are essential, but response capability is what ultimately defines outcomes.
This is where solutions like Pinpoint come into focus. Designed for healthcare environments, Pinpoint’s product enables staff to trigger immediate assistance without relying on complex systems or continuous tracking. In situations where response time directly affects safety, having a simple and reliable way to call for help becomes essential.
FAQ’s
Why is workplace violence increasing in healthcare?
Workplace violence in healthcare is rising due to a combination of factors like higher patient volumes, staffing shortages, mental health challenges, and substance-related cases. These conditions create high-stress environments where situations can escalate quickly if not managed properly.
What are Joint Commission workplace violence prevention requirements for 2026?
The Joint Commission expects hospitals to have a structured workplace violence prevention program in place. This includes risk assessments, incident reporting systems, staff training, and clear response protocols. In 2026, the focus is on showing that these processes are actively implemented and documented, not just written as policies.
Why do workplace violence incidents go unreported?
Many incidents go unreported because staff see them as part of the job or feel reporting takes too much time. In some cases, there is also concern that nothing will change after reporting, which discourages consistent documentation.
Where does workplace violence happen most in hospitals?
It happens most often in emergency departments, behavioral health units, and during patient transitions like admission or discharge. These are the points where stress, uncertainty, and time pressure are highest, which increases the likelihood of escalation.
- The Growing Crisis: Workplace Violence in Healthcare
- Workplace Violence Facts Every Hospital Leader Should Know
- Common Workplace Violence Examples in Healthcare Settings
- Why Workplace Violence Prevention is Now a Regulatory Priority
- Joint Commission Workplace Violence Prevention Requirements (2026)
- Step-by-Step Workplace Violence Prevention Framework
- The Role of Technology in Workplace Violence Prevention
- Closing
- FAQ’s
Author:
Jordan Belous
Chief Marketing Officer of Pinpoint North America, where she leads marketing strategy, brand development, and digital growth initiatives. She earned a Bachelor of Science in Allied Health with a concentration in physical therapy sciences from the University of Tampa, bringing a unique interdisciplinary perspective that blends healthcare knowledge with modern marketing strategy.
Jordan writes about workplace violence prevention in healthcare, nurse safety, staff wellbeing, and emerging healthcare technologies that support frontline teams. Her work explores how hospitals and behavioral health facilities can build safer environments, reduce burnout and turnover, and implement safety systems that protect staff while preserving trust and dignity.
She is also the Chief Executive Officer of Whip Pediatric Cancer, a nonprofit dedicated to supporting children battling cancer and raising awareness and funds for pediatric cancer. Through her work with Whip, Jordan regularly visits pediatric cancer patients in hospitals and spends time alongside patients, families, and the clinicians who care for them. These experiences place her directly beside nurses and healthcare teams every day and reinforce her belief that the people providing care deserve to feel just as safe as the patients they serve.
Her experiences with Whip and her work at Pinpoint are closely connected, both driven by her deep respect for nurses and frontline healthcare workers. Seeing firsthand the compassion, resilience, and critical role nurses play has strengthened her commitment to advocating for safer healthcare environments and ensuring that those who dedicate their lives to caring for others have the protection and support they deserve.