
Workplace Violence Prevention in Healthcare: OSHA, Compliance, and Alert Systems

Let’s be real for a second.
If you work in healthcare, you don’t need a study to tell you violence is getting worse. You’ve felt the tension in the hallways. You’ve seen colleagues brace themselves before walking into certain rooms. You’ve probably been the one holding your breath, hoping today wouldn’t be the day something happened.
But here’s what the data actually says: healthcare and social assistance workers experience violence-related injuries at a rate of 14.2 per 10,000 full-time employees. Compare that to the private industry average of 3.1, and we’re talking about nearly five times the risk. And this isn’t a new problem or a temporary spike, it’s been climbing steadily for over a decade.
If you’re a facility administrator, a safety director, or a nursing leader, you already know the weight of this. You’re the one fielding the calls, reviewing the incident reports, and trying to figure out how to keep your team safe while also keeping the lights on. Building a workplace violence prevention plan isn’t optional anymore but the foundation of protecting your people, your reputation, and your bottom line.
In this guide, we’ll walk through what OSHA actually expects (and what they don’t), what the Joint Commission is looking for during surveys, which state laws pack a real punch, and what alert technology hospitals are putting in place right now to keep staff safe.
Why Is Workplace Violence in Healthcare Getting Worse?
You probably don’t need a study to tell you that violence in healthcare is getting worse. You’re living it. But here’s what the data actually says and it’s pretty alarming.
Healthcare workers account for 73% of all nonfatal workplace injuries caused by violence in the U.S. Between 2011 and 2022, general hospitals saw a 158% increase in violence-related injuries. That’s not a random spike; it’s a decade-long breakdown in how we’re protecting our people. Patient acuity is up, EDs are flooded with mental health crises, staffing shortages leave fewer people managing volatile situations, and long wait times turn frustration into danger.
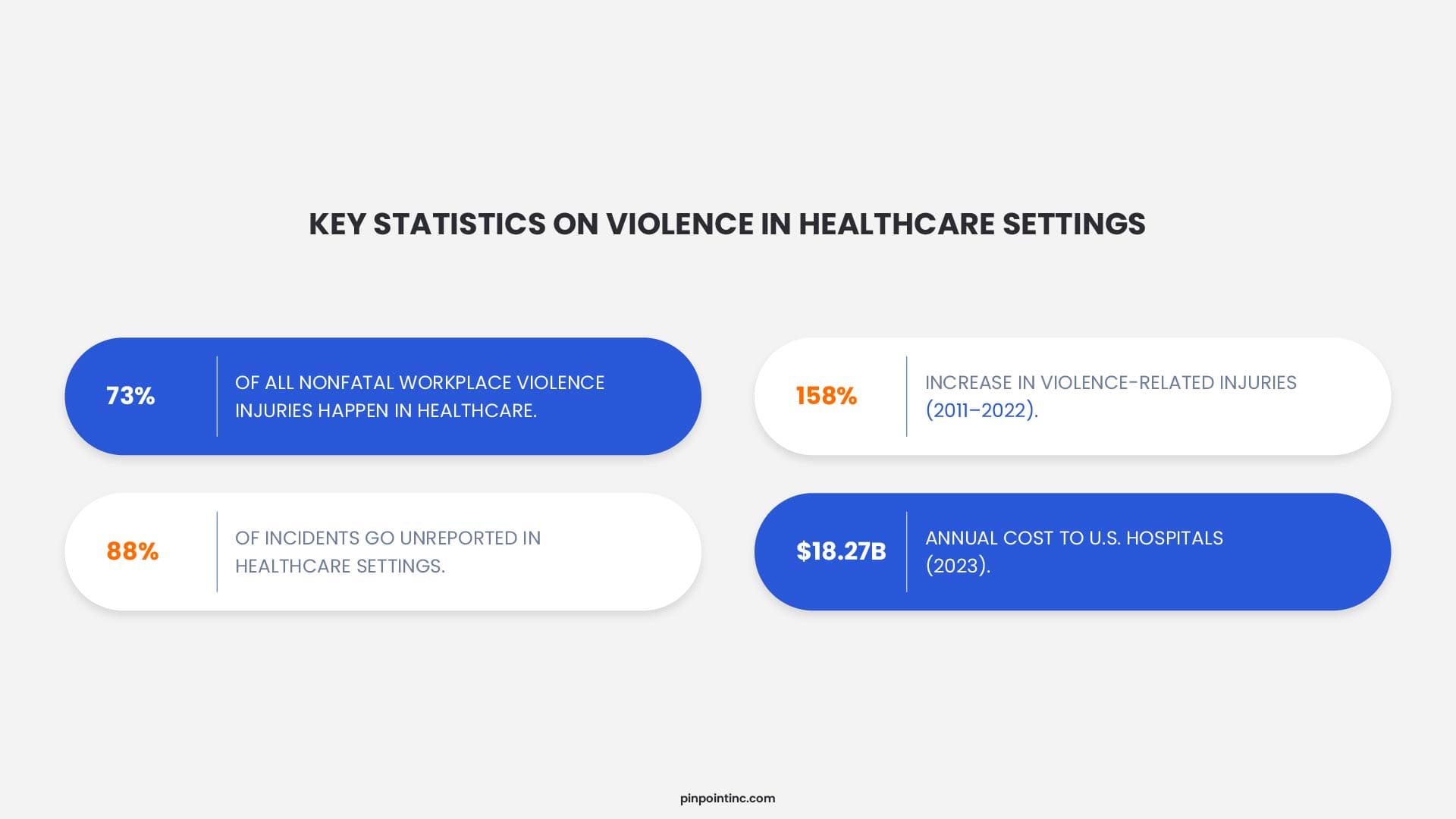
Here’s the kicker: most of it goes unreported. Up to 88% of incidents never get reported, and only 31.7% of nurses have clear reporting mechanisms. So your injury logs? Probably just the tip of the iceberg. Staff often hesitate to file reports because they feel nothing will change, or they simply don’t have time between back-to-back patient loads. That silence creates a dangerous blind spot for leadership.
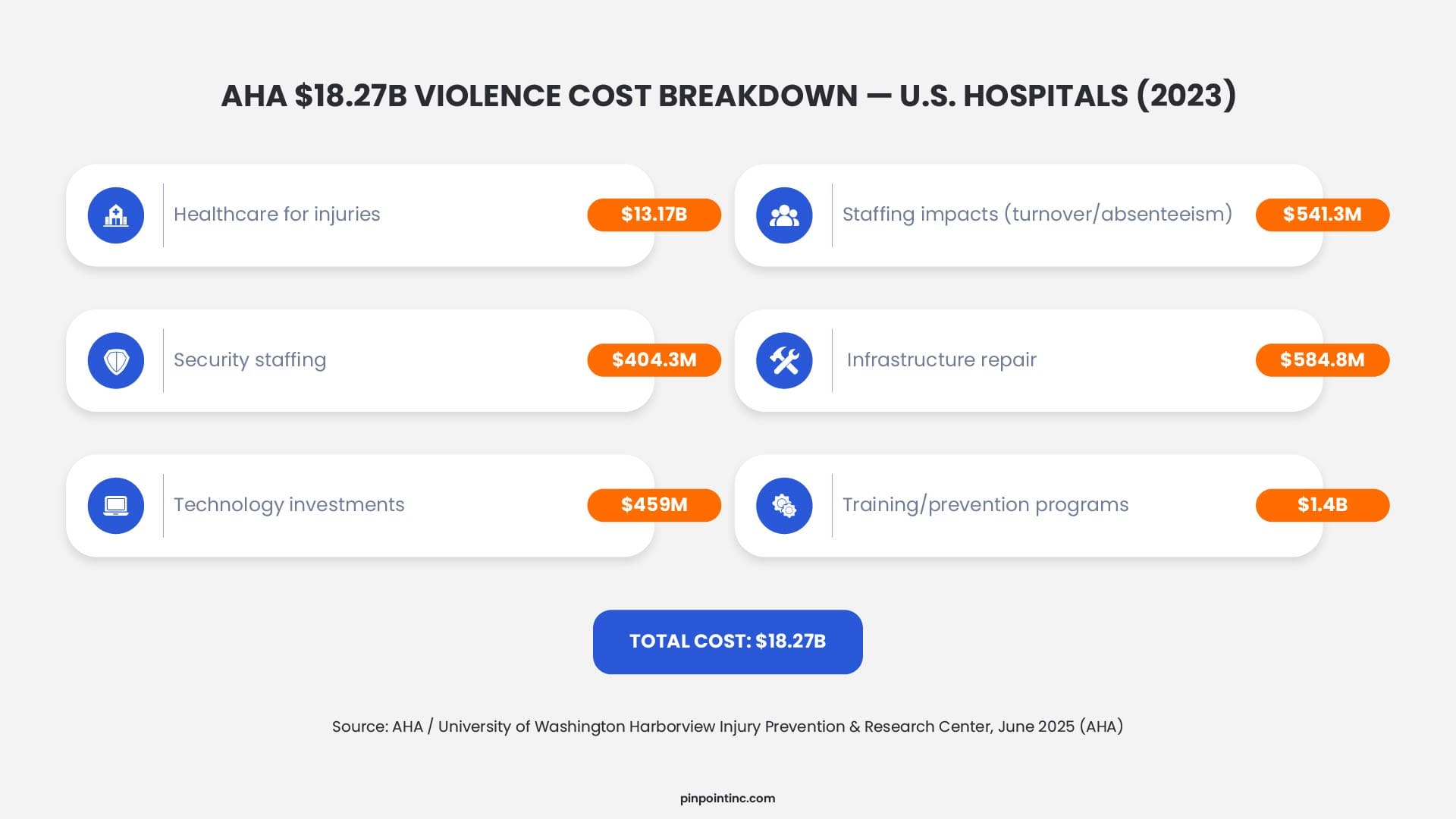
The financial toll is staggering, $18.27 billion in 2023, with $541 million tied to turnover. Replacing one RN costs $60,090; a typical hospital loses $5.19 million annually to turnover. And that’s just the direct costs. When you factor in lost productivity, temporary staffing, and the hit to team morale, the real number climbs even higher. Want to see your facility’s cost? Try our nurse turnover calculator.
Here’s what’s interesting: facilities with the highest violence rates also have the weakest alert infrastructure. That tells us technology is something we can actually control. While you can’t fix staffing shortages or patient acuity overnight, you can implement systems that give staff a lifeline in moments of danger, and that’s a variable worth investing in.
What Does Federal OSHA Currently Require for Healthcare Workplace Violence Prevention?
Here’s the honest answer: not enough. Federal OSHA has no enforceable standard specifically governing workplace violence prevention in healthcare as of 2026. The agency’s proposed rule moved to Long-Term Action status in OSHA’s Spring 2025 regulatory agenda, meaning no federal standard is expected within the next 12 months at minimum (EHS Leaders, 2025).
That said, OSHA enforcement still happens without a dedicated standard. OSHA has cited healthcare employers under the General Duty Clause (Section 5(a)(1)) for failing to protect workers from violence when it’s a recognized hazard. The standard OSHA applies in these citations looks at whether the employer:
- Recognized that workplace violence was a known hazard at the facility
- Had feasible means to reduce or eliminate the hazard
- Failed to implement those means
So even without a formal rule, any hospital, behavioral health center, or residential care facility that ignores documented assault patterns faces genuine enforcement exposure. OSHA’s 2016 guidance document on workplace violence in healthcare, though voluntary, lays out a program framework that inspectors use as a reference baseline during investigations.
A Quick Insight
OSHA's Long-Term Action status is often misread as “they’ve dropped the rule” — but they haven’t. It means the rulemaking timeline is indefinite, but General Duty Clause enforcement is ongoing. Facilities that assume no rule means no risk are misreading the regulatory environment. The citation and litigation record from 2020 to 2024 shows continued healthcare WPV enforcement actions without any dedicated standard.
The practical implication is this: voluntary compliance with OSHA’s guidelines isn’t truly voluntary if your facility is in a state with an OSHA-approved State Plan. California, Washington, Oregon, and Michigan are among the 29 State Plans currently in effect, where state agencies have authority to set standards that meet or exceed the federal baseline. California has already done exactly that with SB 553, which took effect July 1, 2024.
How Do You Build a Workplace Violence Prevention Plan That Meets OSHA Requirements?
A Workplace Violence Prevention Plan is the compliance cornerstone recognized by every major framework: OSHA’s 2016 guidance, the Joint Commission’s Environment of Care standards, and California’s SB 553. Employers with a documented, implemented WVPP are better positioned in both regulatory audits and litigation. OSHA’s guidance identifies five core elements that every effective workplace violence prevention program must include.
What Are the 5 Required Elements of a Workplace Violence Prevention Program?
- Management commitment and worker participation. Senior leadership must visibly endorse the plan and allocate real resources. Nurses and frontline staff should be involved in writing and updating it. They’re the ones who know where the gaps actually are.
- Worksite analysis and hazard identification. This requires a formal assessment of where, when, and how violence occurs. Review incident logs, near-miss reports, workers’ compensation claims, and staff surveys. High-risk zones like emergency departments, waiting rooms, parking structures, and psychiatric units need unit-specific protocols.
- Hazard prevention and control. Physical controls matter: secured access, de-escalation zones, adequate lighting, clear sightlines. Controls must also include staffing ratio thresholds, visitor management policies, and wearable panic button technology that lets staff summon help instantly. This is where technology becomes a critical layer of staff safety in hospitals.
- Safety and health training. Every employee who interacts with patients must receive training on de-escalation, how to recognize escalating behavior, and how to activate the facility’s alert system. Training must be documented, role-specific, and refreshed at least annually.
- Recordkeeping and program evaluation. OSHA requires that incidents be logged per 29 CFR 1904. Your WVPP must specify how incidents are documented, reviewed, and used to update the program. Incident rates, near-miss reports, and staff survey results are all part of a credible, auditable program.
How Do You Conduct a Workplace Violence Hazard Assessment?
Start with a physical walkthrough of every unit and common area. Map the locations where incidents have occurred in the past three years. Then layer in staff interviews. Ask nurses specifically where they feel most at risk and during which shifts. Cross-reference those responses with your incident log.
The goal isn’t a flawless document. It’s a living record that demonstrates you took the hazard seriously, investigated it systematically, and put controls in place. That documented process is what protects the facility in OSHA inspections and civil litigation.
Which State Laws Are Driving Workplace Violence Compliance in Healthcare?
State-level mandates are filling the federal compliance gap fast. For multi-state health systems, the compliance picture is now a patchwork of standards with real enforcement teeth. California leads the way with the most comprehensive law, but other states are quickly following suit.
State-level mandates are filling the federal compliance gap fast, and California is setting the bar high with penalties up to $25,000 per serious violation. For multi-state health systems, the compliance picture is now a patchwork of standards with real enforcement teeth. California leads the way with the most comprehensive law, but other states are quickly following suit.
California SB 553: The Most Comprehensive State Standard in Effect
California’s SB 553 is the most comprehensive workplace violence prevention law enacted in the United States as of June 2026. Signed on September 30, 2023 and enforceable beginning July 1, 2024, it requires every California employer to implement a written Workplace Violence Prevention Plan specific to each work site. For healthcare specifically, Cal/OSHA must adopt an industry-specific standard by December 31, 2026.
California SB 553 requires employers to maintain a written WVPP that’s specific to each physical work site, train all employees on the WVPP before and during initial assignments, maintain a violent incident log for every workplace violence incident, review and update the WVPP after each incident and at least annually, and involve employees and their representatives in developing and reviewing the plan. The penalty exposure is concrete. Cal/OSHA can issue citations with fines up to $25,000 per serious violation under Labor Code Section 6401.9. Failure to maintain a compliant WVPP is an affirmative violation, not just a paperwork gap.
Alyssa's Law and the Healthcare Compliance Pipeline
Alyssa’s Law, first enacted in New Jersey (2019) and Florida (2020), requires public schools to implement silent panic alert systems that connect directly to law enforcement. As of 2026, 11 states have enacted versions of Alyssa’s Law or similar school safety legislation. Why does a school safety law matter for healthcare? Because it establishes a legal and cultural precedent for silent alert technology as a regulatory requirement rather than an optional upgrade.
Safety directors at healthcare facilities in states with Alyssa’s Law requirements are already being asked by administrators: “Why don’t we have something similar for our staff?” The legislative pattern from school safety to healthcare safety typically runs 3-5 years, meaning facilities with existing staff safety in hospitals infrastructure are ahead of the next compliance cycle.
How Do Alert Systems Support Preventing Workplace Violence in Healthcare?
Alert technology is the operational layer that makes a Workplace Violence Prevention Plan work in real time. A written policy won’t stop an assault in progress, however, the speed of the response after an incident begins determines outcomes, and that depends entirely on whether staff can summon help instantly.
Wearable Panic Buttons vs. Fixed Duress Alarms: What's the Practical Difference?
Fixed duress alarms, like under-desk buttons and wall-mounted call stations, have a fundamental limitation. They only work when the person in danger is within reach of the device. But nurses move constantly. They’re in patient rooms, hallways, stairwells, and parking structures. A fixed alarm simply doesn’t travel with them.
Wearable panic buttons solve that problem. A staff member wears a small badge or clip-on device. When threatened, they press it. The alert fires with room-level location data, not GPS coordinates, but a room or zone designation that tells responders exactly where to go.
The distinction matters for two important reasons. First, GPS-based tracking systems raise serious staff privacy concerns in healthcare settings. Continuous passive location monitoring of employees creates legal and HR complications that most facilities want to avoid. Non-tracking wearable systems alert on demand without logging staff movements between presses. Second, room-level accuracy is often more actionable for an internal response team than a GPS coordinate that still requires physically searching an area. If you’re evaluating different options, understanding the various types of healthcare panic button systems can help you make the right choice for your facility.
Which Facility Types Benefit Most from Wearable Alert Systems?
High-risk environments, including behavioral health units, emergency departments, psychiatric hospitals, and residential rehabilitation centers, benefit most from wearable alert systems. In these settings, a fast staff alert network isn’t optional. It’s a core safety control. Nurses and healthcare workers in these units face volatile situations daily, and every second counts when a threat escalates.
Facilities that integrate wearable alert systems into their WVPP can document the technology as a specific hazard control in their hazard assessment. That matters for compliance. “Staff are trained to use the phone in an emergency” is a weak control. “Staff wear real-time alert devices that notify security within seconds and pinpoint their location to the room level” is a strong one.
OSHA and the Joint Commission both look for specific, documented controls, not general statements about awareness. When you’re building your workplace violence prevention program, having that level of specificity in your hazard assessment makes all the difference during audits and inspections.
How Do You Know Whether Your Workplace Violence Prevention Program Is Working?
A workplace violence prevention program that isn’t measured isn’t really a program at all. It’s just a document collecting dust on a shelf. OSHA’s guidance and the Joint Commission both require that incident data be analyzed and used to continuously improve the plan. Without measurement, you’re operating blind.
So how do you know if your program is actually working? Here are the key metrics and methods that matter most for healthcare facilities serious about staff safety.
Track Incident Rates by Unit and Shift
Start with the basics: track incident rates per 100 full-time employees, broken down by specific units and shifts. This granularity matters because violence doesn’t happen uniformly across a facility. Your emergency department likely faces different risks than your behavioral health unit, and night shifts may see different patterns than day shifts.
Compare your rates quarter over quarter. Are they trending up, down, or holding steady? Then benchmark against BLS SOII data for your specific facility type. If your behavioral health unit is above the national average for similar facilities, it warrants an emergency program review.
Why This Matters For Compliance
Benchmarking converts raw numbers into actionable signals. It tells you whether you're performing worse than comparable facilities or better. That distinction is critical when OSHA or the Joint Commission comes knocking.
Monitor Near-Miss Reports Separately
Near-miss reports are your early warning system. A unit that files 12 near-miss reports before a formal injury occurs is communicating that conditions are deteriorating. If your reporting system doesn’t capture near-misses separately from formal injury logs, you’re reading the dashboard after the crash.
Create a culture where near-misses are reported without fear of blame. Staff need to know that reporting a close call isn’t admitting failure. It’s preventing the next incident. When near-miss reports spike, investigate immediately. That’s your chance to intervene before someone gets hurt.
Survey Staff About Perceived Safety
Formal injury metrics only tell you what already happened. Staff perception surveys tell you what’s coming.
Survey your staff twice a year about perceived safety. Ask specific questions:
- Do you feel safe during your shifts?
- Are you confident in the facility’s emergency response?
- Do you know how to activate the alert system?
- Would you recommend this facility to a colleague?
Here’s why this matters: Staff retention surveys that include violence-related questions give you a leading indicator that formal injury metrics miss. A drop in perceived safety scores often precedes a spike in formal incident rates by two to three reporting periods. When staff feel unsafe, they start leaving, and the cost of replacing one registered nurse averages $60,090.
If you have a wearable alert system, track response times religiously. How long does it take for a responder to reach a staff member who activates a duress alert? That metric is the clearest operational test of whether your alert infrastructure is actually performing as designed.
Summing Up
Workplace violence in healthcare isn’t a new problem, but the regulatory and financial pressure to address it formally has never been higher. California is enforcing a Workplace Violence Prevention Plan mandate right now, and the Joint Commission is actively citing hospitals that lack documented programs.
We’ve covered what OSHA requires and what it doesn’t, what the Joint Commission expects during surveys, which state laws carry real enforcement teeth, and what alert technology hospitals are using to protect staff right now. We’ve walked through the five core elements of an effective WVPP, the difference between fixed and wearable alert systems, and how to measure whether your program is actually working.
Facilities getting this right share a common pattern: a written, site-specific Workplace Violence Prevention Plan, consistent staff training with documented records, a technology layer that gives nurses a real way to summon help in seconds, and a measurement system that tracks whether any of it is working. If you’re building or updating your program, start with the hazard assessment. That single step transforms a compliance document into an actual prevention program.
Pinpoint helps healthcare facilities implement wearable alert technology that integrates seamlessly with your WVPP, giving your staff a lifeline in moments of danger while keeping you ahead of regulatory requirements.
Ready To See How It Works?
Schedule a demo today and let's talk about protecting your people.
FAQ’s
What exactly counts as workplace violence in healthcare?
Workplace violence in healthcare includes any act or threat of physical violence, harassment, intimidation, or other threatening behavior that occurs at the work site . The National Institute for Occupational Safety and Health defines it as violence ranging from verbal abuse to physical assault and even lethal acts directed at employees while on duty . It’s more than just physical attacks. It includes verbal threats, bullying, sexual harassment, and psychological abuse .
Is a Workplace Violence Prevention Plan legally required in healthcare?
At the federal level, no specific OSHA standard mandates a written WVPP for healthcare as of 2026. The proposed rule is in Long-Term Action status. However, California SB 553 (effective July 1, 2024) requires all California employers to maintain a written WVPP, with fines up to $25,000 per serious violation. The Joint Commission requires accredited hospitals to have workplace violence policies and programs. And federal OSHA can still cite healthcare employers under the General Duty Clause for recognized, preventable hazards. Facilities without a written program carry compliance, accreditation, and litigation risk simultaneously.
Does workplace violence affect nurse retention?
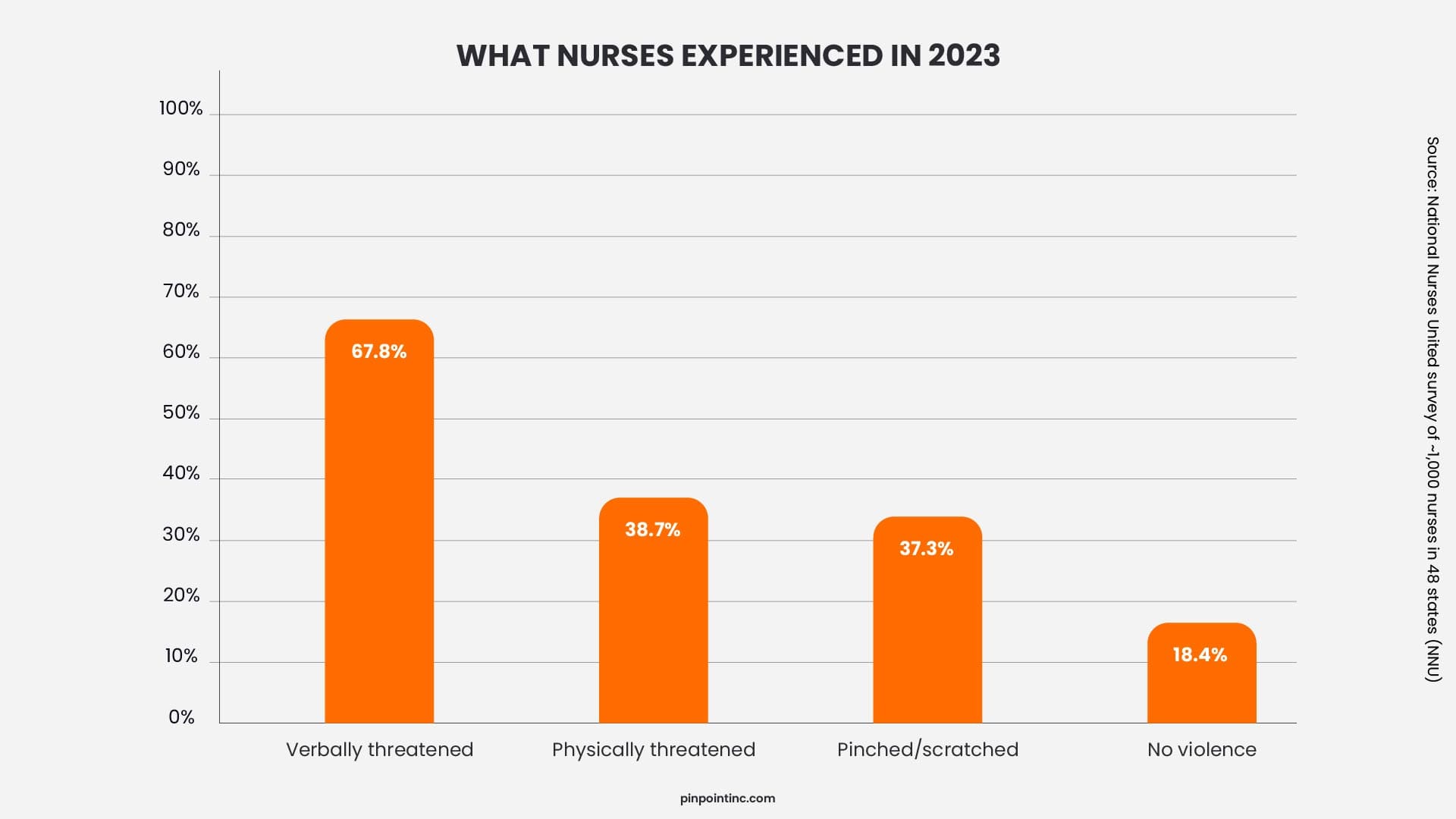
Yes, significantly. In NNU’s 2024 survey of approximately 1,000 nurses, 60% of those who experienced violence considered leaving their jobs, and a portion had already changed positions (NNU, 2024). Given that replacing one registered nurse costs an average of $60,090 (NSI National Health Care Retention Report, 2026), the financial case for violence prevention investment is straightforward: any reduction in violence-driven turnover pays for itself quickly.
What's the difference between a duress alarm and a panic button in a hospital?
The terms are often used interchangeably, but there’s a meaningful distinction. A panic button is typically a device or app that sends an alert to security or staff when activated. A duress alarm specifically signals that someone is in danger under coercion, and they may be unable to speak or act visibly. In hospital settings, the key performance criteria are the same: how fast does the alert reach a responder, and how accurately does it communicate location? Fixed duress alarms only help when staff are within reach of a wall unit. Wearable devices solve the mobility problem.
What technology should be included in a hospital workplace violence prevention program?
Effective programs combine several technology controls: badge-based access control, visitor management systems, security camera coverage in high-risk areas, a staff duress alert system (wearable or fixed), and an incident documentation platform. For wearable alert systems specifically, look for room-level location accuracy without passive GPS tracking, fast single-press activation, integration with existing security dashboards, and clear documentation of responder roles within the program. The technology is only as good as the responder protocol behind it.
- Why Is Workplace Violence in Healthcare Getting Worse?
- What Does Federal OSHA Currently Require for Healthcare Workplace Violence Prevention?
- How Do You Build a Workplace Violence Prevention Plan That Meets OSHA Requirements?
- Which State Laws Are Driving Workplace Violence Compliance in Healthcare?
- How Do Alert Systems Support Preventing Workplace Violence in Healthcare?
- How Do You Know Whether Your Workplace Violence Prevention Program Is Working?
- Summing Up
- FAQ’s
Author:
Jordan Belous
Chief Marketing Officer of Pinpoint North America, where she leads marketing strategy, brand development, and digital growth initiatives. She earned a Bachelor of Science in Allied Health with a concentration in physical therapy sciences from the University of Tampa, bringing a unique interdisciplinary perspective that blends healthcare knowledge with modern marketing strategy.
Jordan writes about workplace violence prevention in healthcare, nurse safety, staff wellbeing, and emerging healthcare technologies that support frontline teams. Her work explores how hospitals and behavioral health facilities can build safer environments, reduce burnout and turnover, and implement safety systems that protect staff while preserving trust and dignity.
She is also the Chief Executive Officer of Whip Pediatric Cancer, a nonprofit dedicated to supporting children battling cancer and raising awareness and funds for pediatric cancer. Through her work with Whip, Jordan regularly visits pediatric cancer patients in hospitals and spends time alongside patients, families, and the clinicians who care for them. These experiences place her directly beside nurses and healthcare teams every day and reinforce her belief that the people providing care deserve to feel just as safe as the patients they serve.
Her experiences with Whip and her work at Pinpoint are closely connected, both driven by her deep respect for nurses and frontline healthcare workers. Seeing firsthand the compassion, resilience, and critical role nurses play has strengthened her commitment to advocating for safer healthcare environments and ensuring that those who dedicate their lives to caring for others have the protection and support they deserve.