
What to Look for Before Buying a Duress Alarm System for Healthcare Facility
A dead battery goes undetected for months, a device loses its connection without anyone knowing, or a hallway alert shows only a floor number instead of a specific room. Your staff presses the button believing help is coming, but help never arrives at the right place, and by the time responders figure it out, the situation has already escalated.
That is not just a technology failure; it is a failure of trust. When trust breaks, nurses stop pressing the button, they handle escalating situations alone, retention drops, and your next Joint Commission surveyor finds gaps in your response time logs.
This guide avoids the same old violence statistics you have already seen and instead gives you eight practical, vendor‑neutral criteria to evaluate any duress alarm system before you sign a contract. Hospital administrators, CNOs, and IT directors can use it as a pre‑purchase checklist, a negotiation tool, and a straightforward framework for keeping staff safe and compliance clean.
Why Most Duress Alarm Purchases Get It Wrong
Healthcare workplace violence costs US hospitals an estimated $18.27 billion annually, according to the American Hospital Association. A 2026 Nurse.org survey found that 27% of nurses were physically assaulted in 2025, and nearly half say safety concerns may drive them to leave their jobs within the next year. Yet most facility leaders still evaluate duress alarm systems like office equipment: price, looks, and a polished demo. The result is a system that technically works but fails staff when it matters most.
The failure patterns are painfully predictable. A pendant that triggers an alert but only shows a building name, not a room number. A Bluetooth badge that works in the lobby but loses accuracy in a metal‑framed behavioral health unit. An alert that reaches security but never makes it to the floor supervisor’s phone. These are not rare failures; they are the documented reality of hospitals that prioritized budget over behavioral health readiness.
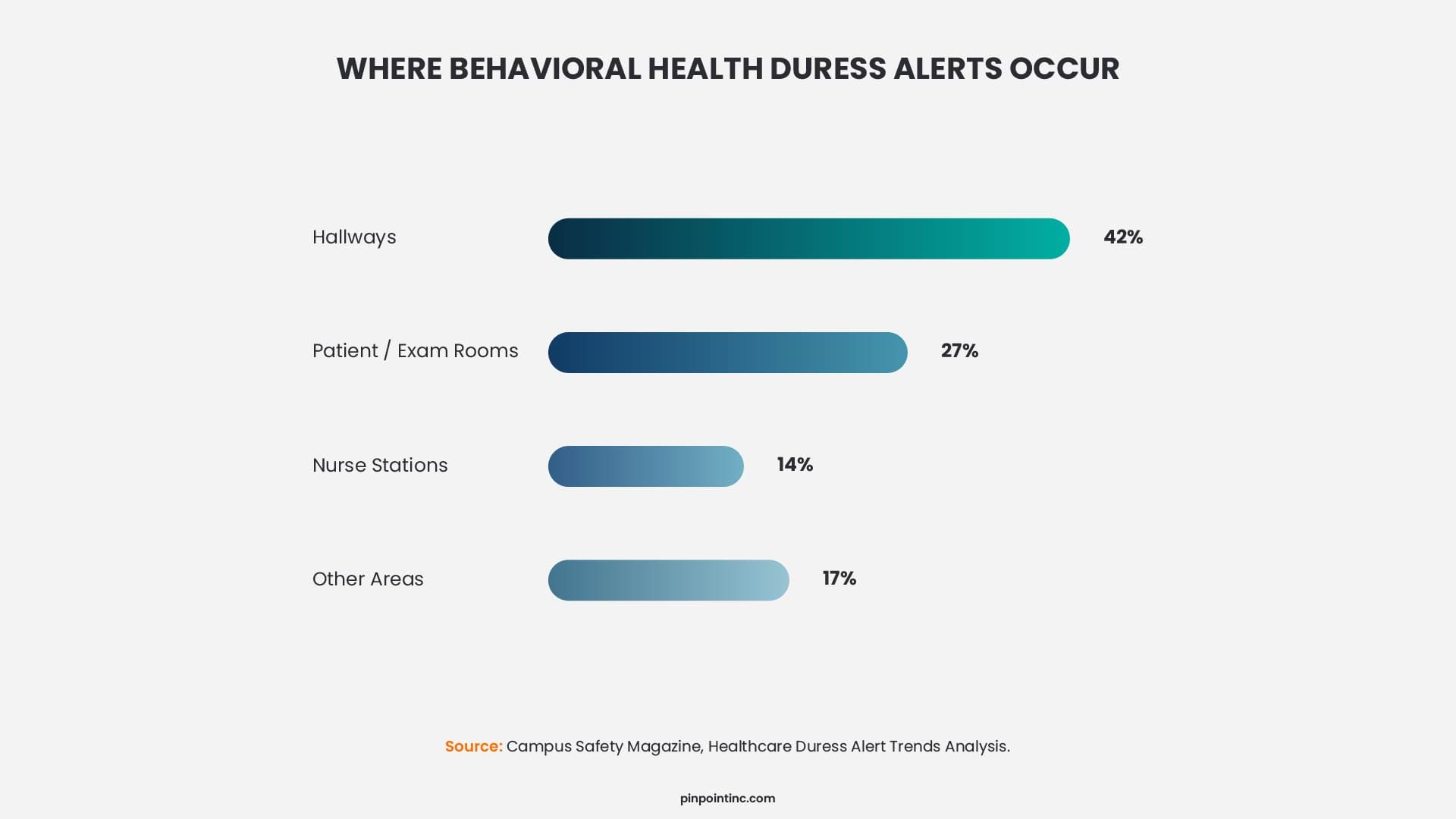
Where do most wearable duress alerts actually originate? Not inside patient rooms, but in corridors, common areas, and transitional spaces where staff interact with patients between fixed locations. A duress alarm system that cannot track movement through these passages with certainty will leave responders guessing which wing or floor. That delay turns a manageable situation into a crisis.
The 8‑Point Checklist: What to Evaluate Before You Buy (Staff Duress Alert System Focus)
Alert speed, device durability, and compliance documentation all matter when evaluating a staff duress alarm system, but they do not matter equally and they do not matter in isolation. Use this checklist to compare any vendor proposal systematically.
1. Location Technology & Accuracy for Healthcare Duress Alerts
Location accuracy determines whether responders reach the right place at the right time. There are three main technologies for hospital duress alert systems, each with different precision levels.
- Infrared (IR) delivers true room-certain accuracy. The signal fires only when a receiver in a specific room picks it up, with no ambiguity. This makes IR the preferred choice for behavioral health duress alarms and emergency departments.
- Bluetooth Low Energy (BLE) provides near-room accuracy of roughly three to five meters at a lower infrastructure cost. However, BLE performance can degrade in metal-rich environments like psychiatric units or older hospital wings.
- Ultra-Wideband (UWB) offers sub-meter precision, but the significantly higher cost often limits it to operating suites or high-value asset tracking rather than staff duress applications.
For emergency departments and behavioral health units, where 42% of alerts occur in corridors and transitional spaces, IR precision is the safer choice for staff duress alert systems. For lower-risk common areas like lobbies or administrative offices, BLE works well.
2. Wi-Fi Independence for Hospital Panic Button Systems
Hospital Wi-Fi is among the most congested radio frequency environments in any building type, with dozens of clinical devices competing for bandwidth on every floor. A hospital panic button that routes alerts through the facility’s wireless network introduces a single point of failure at exactly the wrong moment. If a network switch goes down, a router becomes overloaded during a high-census period, or an access point loses power, the system may go completely silent when someone presses their button for help.
Wi-Fi independent duress systems communicate through dedicated hardwired receiver infrastructure or private wireless mesh networks, which means no Wi-Fi dependency, no Bluetooth interference, and no cellular requirement. A wearable panic button built on this architecture will fire an alert even when the hospital network is offline.
Ask vendors directly: “What happens to alert delivery if the hospital Wi-Fi is down?” If the answer includes “alerts may be delayed” or “coverage may be reduced in some areas,” that is a disqualifier for emergency departments, behavioral health units, and any high-risk area where immediate response is non-negotiable.
Healthcare is the most cyber-targeted industry in the United States, accounting for 27% of all data security incidents across every sector.
3. Alert Delivery Pathways for Duress Alarm Systems
An alert that only reaches the security desk is not an enterprise-grade duress notification system. Effective response requires simultaneous notification across every device that a relevant responder carries or monitors.
At minimum, a clinical alarm system should deliver alerts to:
- Mobile apps for iOS and Android so staff on the floor receive alerts instantly
- Desktop PC software for supervisors monitoring from a central station
- LCD display panels in common areas for visual awareness
- Over-door visual lights for non-verbal indication during active situations
- Audible sounders with customizable tones for different alert levels
Systems that only ring a security radio, or that require staff to download a third-party app outside the platform, create unnecessary response gaps. Ask vendors to demonstrate all active notification channels working at the same time, not just one channel in isolation.
4. Behavioral Health Hardware Standards for Ligature Resistant Devices
For psychiatric inpatient units and behavioral health wings, hardware requirements depend on who wears the device and where it is used.
For staff‑worn devices: A staff duress alert system can use a wearable badge or pendant because staff are responsible adults who can remove the device when entering a high‑risk patient room. However, the device should use a breakaway lanyard or clip to a lapel or pocket, not a fixed loop.
For patient‑facing hardware: Any device left in a patient room, mounted on a wall, or worn by a resident must be fully ligature resistant. This includes receiver brackets, wall plates, fasteners, display housings, over‑door lights, and any other mounted component. No loops, hooks, or hanging elements that could support self‑harm are permitted.
For both categories: Hardware must also be antimicrobial to survive high‑grade cleaning chemicals and tamper resistant using security screws to prevent removal or destruction.
5. Analytics & Compliance Documentation for Hospital Duress Alert Systems
The Joint Commission’s workplace violence prevention standards were updated in 2025 and are now fully enforced across all accredited facilities in 2026. These standards require hospitals to maintain documented evidence of their violence prevention program, including incident hotspot data, response time records, and usage patterns. A duress alarm system without a management analytics portal leaves you exposed during your next accreditation review.
Look for a compliance portal that logs the following data points:
- Alert origin by specific location and timestamp
- Response time measured from button press to acknowledgment
- Department level usage frequency to identify trends
- Trend analysis over weeks, months, or quarters
This data does more than satisfy surveyors. It drives continuous improvement, if your analytics portal shows that the third floor med surg wing generates 60% of all duress alerts, your safety committee knows exactly where to invest next in training, staffing, or environmental changes.
6. Programmable Multi-Button Design for Duress vs Panic Scenarios
Single-button systems force staff into a binary choice. Press it and trigger a full emergency response, or do not press it and handle the situation alone. Most real incidents, such as a confused patient escalating or a difficult family member in a waiting room, fall somewhere in the middle.
Systems with two programmable buttons allow staff to signal for two different levels of need. One button can request assistance, meaning send backup but keep the response calm and measured. The other button can signal an emergency, meaning urgent, all hands, immediate response. This distinction between duress vs panic button functionality dramatically reduces both under-use of the system and alert fatigue across the facility.
Alert fatigue is a documented failure mode in single-button deployments. When every button press triggers a security lockdown level response, floor staff stop pressing the button for anything short of a physical altercation. A system that offers both assistance and emergency options gives staff a reason to use the device before a situation spirals out of control.
7. Multi-Facility & Enterprise Scalability
Systems that work perfectly in a 50 bed facility often break down at enterprise scale. For large health systems operating multiple buildings, campuses, or separate facilities, the scalable duress alarm platform must support centralized management. That means a single management portal with the ability to segment by facility, floor, or department, without requiring separate software installations or separate vendor contracts per site.
Ask vendors about maximum device counts, multi-building configurations, and how the system handles a staff member moving across a campus between buildings. Expansion pathways matter. A system that requires a full infrastructure replacement just to add a new wing will become a budget problem faster than you expect.
8. Total Cost of Ownership & Vendor Support
The per-device price on a vendor quote is rarely the number that matters. Total cost of ownership for a discreet duress alarm system includes hardware such as badges, receivers, and displays; installation costs like receiver density surveys, cabling, and commissioning; software licensing including annual SaaS fees, portal access, and integrations; and ongoing support such as 24/7 helpline availability, maintenance contracts, and replacement device service level agreements.
A system that costs $30,000 less upfront but lacks 24/7 support, charges per-integration fees, and requires full infrastructure replacement to expand will cost significantly more over a five year span. Always request itemized proposals that separate hardware, installation, licensing, and support into distinct line items so you can compare vendor quotes honestly.
CTA: For a deeper dive into real-world applications, explore our complete resource library for more insightful guides.
Comparing Location Technologies: IR, BLE, UWB, and Hybrid
The location engine is the most consequential technology decision in any duress alarm purchase. Responders arriving at the wrong room, or even the wrong wing, during a behavioral health crisis is not a simple system error. It is a staff safety failure.
Here is how the four main technologies compare across criteria that actually matter for healthcare.
| Technology | Location Precision | Wi-Fi Required | Infrastructure Cost | Best For |
|---|---|---|---|---|
| Infrared (IR) | Room-certain | No | Medium | Behavioral health, ED, ICU |
| BLE (Bluetooth Low Energy) | Near-room (3–5 meters) | Often yes | Low | Common areas, lower-risk floors |
| UWB (Ultra-Wideband) | Sub-meter | No | High | OR suites, high-value asset areas |
| Hybrid IR + BLE | Room-certain where it counts | No in IR zones | Medium | Enterprise campuses with tiered coverage |
The dominant deployment pattern in 2026 is tiered coverage:
- Infrared (IR): Placed in emergency departments, behavioral health units, and inpatient wings where precision is life-critical.
- Bluetooth Low Energy (BLE): Utilized in lobbies, parking structures, and administrative areas where near-room accuracy is sufficient and cost efficiency matters more.
How Pinpoint Inc Meets Every Criterion on the Checklist
Most duress healthcare systems check only a few of the boxes we have covered. Pinpoint was built differently. It is the only staff duress platform designed exclusively for US healthcare environments, not retrofitted from commercial security or education deployments. The system delivers room-certain location using infrared with non-RTLS system (so privacy is protected), operates independently of hospital Wi-Fi (reducing cyberattack risks and single points of failure), and includes ligature resistant hardware as a standard feature, not an upsell. The two button design lets staff request assistance or signal an emergency, and the built in analytics portal provides Joint Commission ready compliance reports.
Pinpoint is easy to wear, easy to use, and built specifically for hospitals, behavioral health units, and residential rehab facilities. That focus is why it checks all eight criteria while others only check a few.
See Pinpoint in Action
Request a live demo to see how Pinpoint performs in your clinical environment.
2026 Key Insight
The dominant deployment pattern in 2026 is tiered coverage. Hospitals are placing IR in emergency departments, behavioral health units, and inpatient wings where precision is life critical. They are using BLE in lobbies, parking structures, and administrative areas where near-room accuracy is sufficient and cost matters more.
Industry Insight
RTLS systems in healthcare are effective for tracking and operational visibility, but their real-world success depends heavily on change management, system complexity, and staff adoption – Source
FAQ’s
Does OSHA require duress alarms in hospitals?
Not exactly, the OSHA has not issued a specific standard that explicitly requires duress alarms. However, OSHA’s workplace violence guidelines for healthcare strongly recommend that all hospitals maintain a comprehensive, system‑wide violence prevention plan. As part of that plan, personal alarm devices worn by staff, duress buttons, or workstation paging systems are frequently cited as effective engineering controls.
Can a single duress alarm system cover both hospital staff and patients?
Yes, the best enterprise platforms handle both on a single infrastructure. Pinpoint Inc supports staff wearables (ID badge-holder panic alarm with two programmable buttons) and patient devices (water-resistant, antimicrobial wrist band call button) on the same alert and analytics platform. This unified approach eliminates the operational complexity of managing separate staff safety and nurse call systems from different vendors.
What is the average battery life of a staff duress badge?
Battery life varies by technology and usage. Most wearable duress badges last between one and three years on a single battery, depending on how often the device is used and whether it includes features like two‑way audio or continuous location tracking. Supervised systems will alert administrators when a device battery is low, so staff are never left with a non‑functional button.
Do duress alarm systems track staff location all the time?
Not all systems do. Some solutions use real‑time location services (RTLS) that continuously track where staff are at all times, which raises privacy concerns for many healthcare workers. However, other systems, including Pinpoint, use infrared or similar technologies that only activate location identification at the exact moment a duress button is pressed. Outside of an active alert, no location data is collected or stored.
Author:
Jordan Belous
Chief Marketing Officer of Pinpoint North America, where she leads marketing strategy, brand development, and digital growth initiatives. She earned a Bachelor of Science in Allied Health with a concentration in physical therapy sciences from the University of Tampa, bringing a unique interdisciplinary perspective that blends healthcare knowledge with modern marketing strategy.
Jordan writes about workplace violence prevention in healthcare, nurse safety, staff wellbeing, and emerging healthcare technologies that support frontline teams. Her work explores how hospitals and behavioral health facilities can build safer environments, reduce burnout and turnover, and implement safety systems that protect staff while preserving trust and dignity.
She is also the Chief Executive Officer of Whip Pediatric Cancer, a nonprofit dedicated to supporting children battling cancer and raising awareness and funds for pediatric cancer. Through her work with Whip, Jordan regularly visits pediatric cancer patients in hospitals and spends time alongside patients, families, and the clinicians who care for them. These experiences place her directly beside nurses and healthcare teams every day and reinforce her belief that the people providing care deserve to feel just as safe as the patients they serve.
Her experiences with Whip and her work at Pinpoint are closely connected, both driven by her deep respect for nurses and frontline healthcare workers. Seeing firsthand the compassion, resilience, and critical role nurses play has strengthened her commitment to advocating for safer healthcare environments and ensuring that those who dedicate their lives to caring for others have the protection and support they deserve.