
RTLS Alternatives for Hospital Staff Safety: Non-Tracking Systems That Deliver Real Results

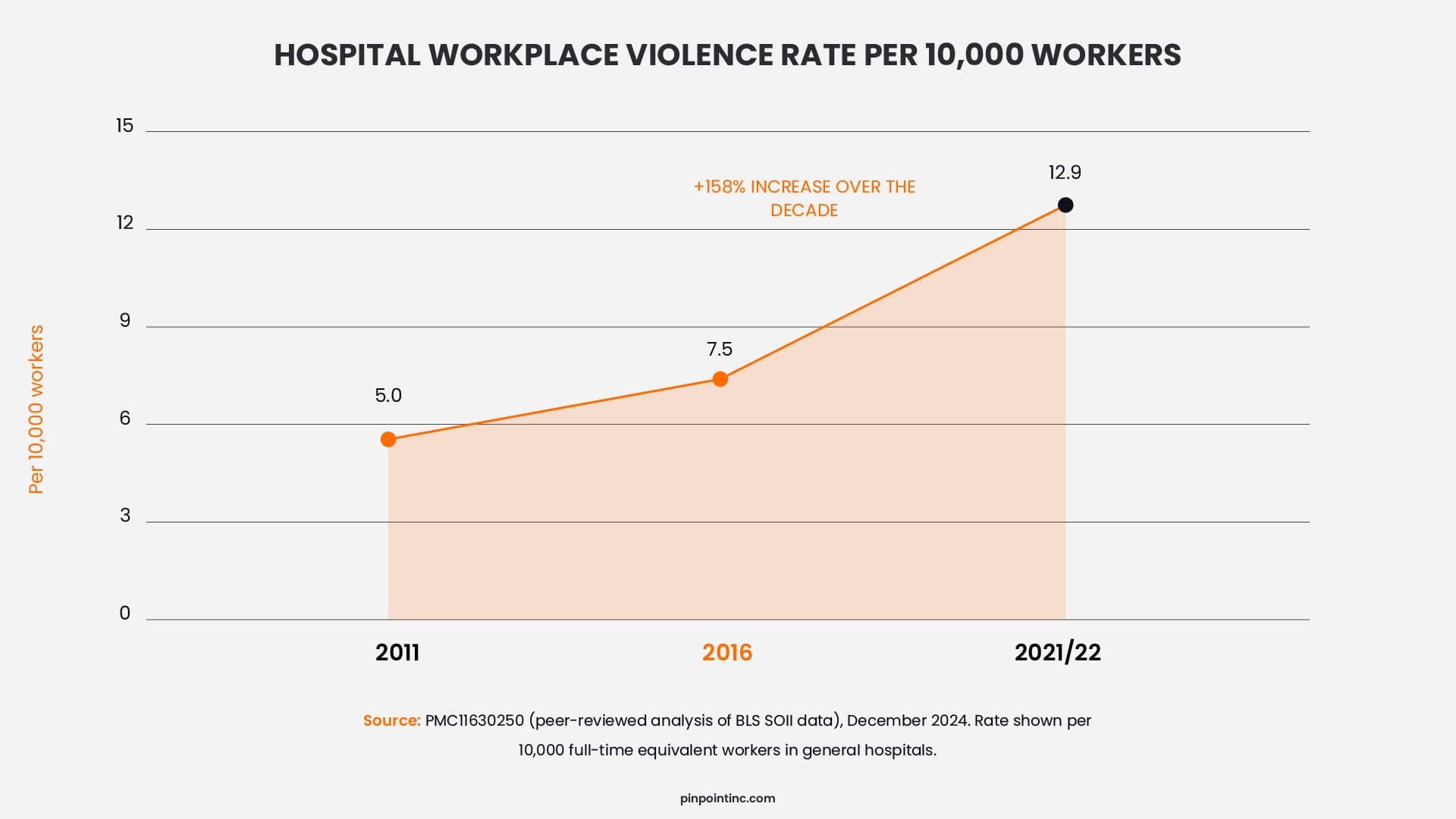
Hospital workplace violence has surged 158% per 10,000 workers over the past decade, according to a 2024 Health Affairs Scholar. Yet the most expensive staff safety technology many hospitals are evaluating may not be the right tool for the problem. Real-time location systems (RTLS) have become a common recommendation for hospital staff protection, but with high infrastructure costs and long deployment timelines, they can leave staff waiting too long for protection they need now.
For staff safety specifically, hospitals have a more focused option. Non-tracking wearable duress systems, including panic buttons that activate only when pressed and collect no continuous location data, can often deploy faster, cost less than full RTLS infrastructure, and reduce privacy concerns because staff are not monitored throughout their shift. And as of January 2026, the Joint Commission’s workplace violence prevention requirements focus on program elements, not a specific RTLS technology mandate.
This guide breaks down viable alternatives to RTLS for hospital staff safety, with cost comparisons, use-case guidance, and a practical framework for building a compliant workplace violence prevention program, whatever technology you choose.
How Serious Is the Hospital Workplace Violence Crisis?
Before comparing RTLS alternatives for hospital staff safety, hospitals need to understand what they are actually solving for. The issue is not simply locating staff on a map, it’s making sure a nurse, clinician, or support worker can call for help quickly, without friction, when a violent or escalating situation occurs.
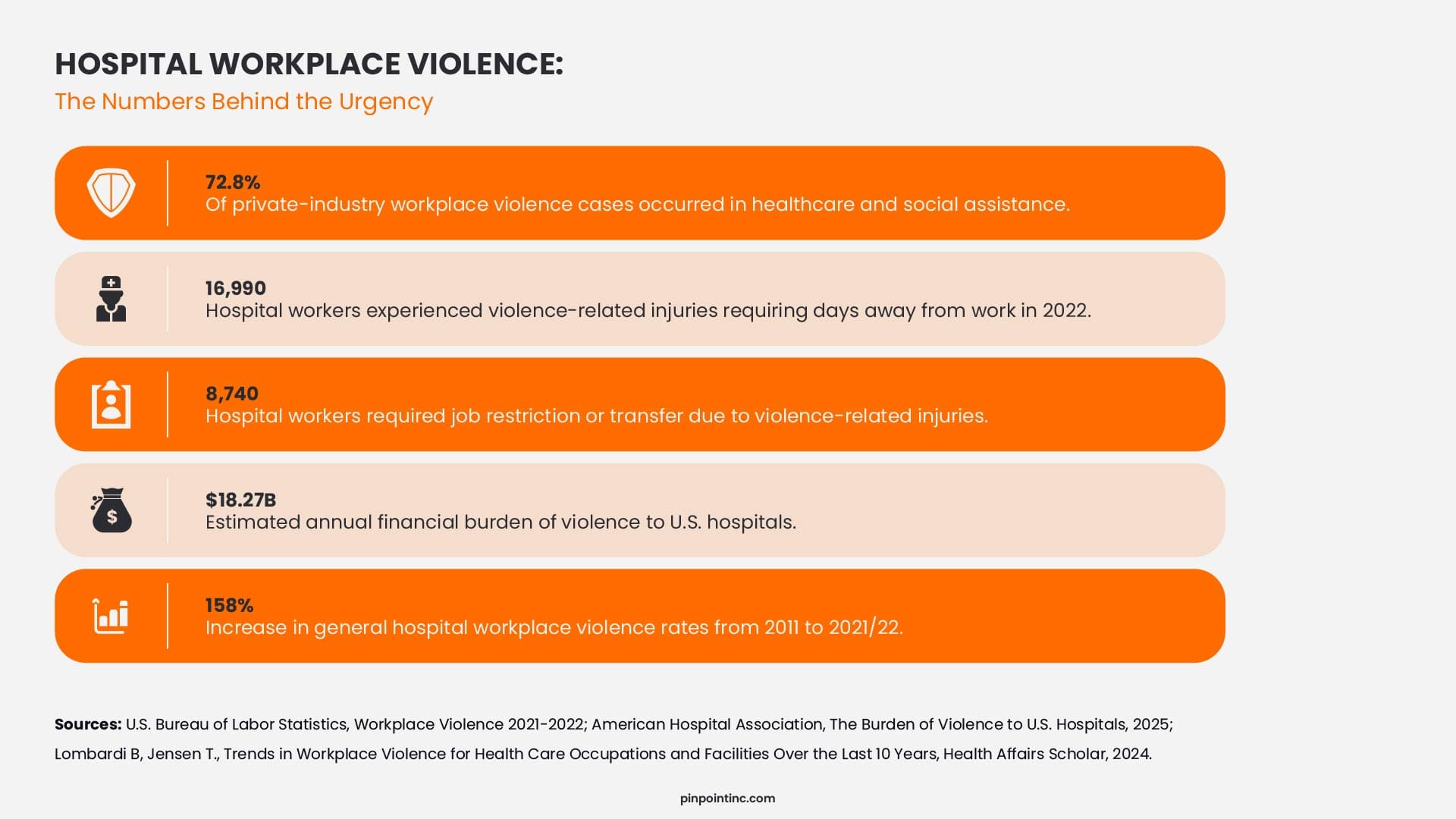
The data makes the priority clear. Hospital workplace violence is increasing pressure on safety teams, clinical leaders, and operations because every delayed response can affect staff confidence, incident outcomes, reporting, and retention. That is why the technology decision has to focus on response speed, ease of use, and staff adoption, not just system complexity.
This is where the RTLS conversation needs more precision. RTLS for hospital staff safety can support location awareness, but continuous tracking is not always required to get help to the right area quickly. For many facilities, non-tracking wearable duress systems offer a more focused way to trigger alerts, notify responders, and support frontline staff without building a full RTLS infrastructure first.
Industry Insight
RTLS systems in healthcare are effective for tracking and operational visibility, but their real-world success depends heavily on change management, system complexity, and staff adoption – Source
What Is RTLS and Why Are Hospitals Buying It for Staff Safety?
When hospitals look for staff safety technology, RTLS often comes up because it promises one thing leaders care about during an emergency: location awareness. RTLS stands for real-time location system, and in healthcare it is used to identify where tagged resources are located inside a facility.
Those tagged resources can include equipment, patients, visitors, and staff wearing RTLS-enabled badges. Hospitals use RTLS for use cases such as locating IV pumps, wheelchairs, crash carts, and beds, monitoring patient transport, supporting wandering-risk patient workflows, and giving teams visibility into staff or asset movement across units.
For staff safety, the use case is narrower. When a nurse is threatened in a hallway at 2 a.m., the priority is fast, discreet alerting, clear responder notification, and enough location context to send help quickly.
Industry Insight
RTLS systems in healthcare are effective for tracking and operational visibility, but their real-world success depends heavily on change management, system complexity, and staff adoption – Source
Why Are Hospitals Reconsidering RTLS for Staff Safety?
Hospitals are not rejecting RTLS entirely. Many still use it for asset tracking, patient flow, and operational visibility. The question is narrower: whether RTLS for staff safety is the best first investment when the goal is fast alerting, staff adoption, privacy protection, and reliable emergency response.
Cost and Deployment Time
RTLS can require a major infrastructure investment, especially when hospitals need room-level or facility-wide coverage. A 100-bed hospital RTLS implementation can cost more than $500,000 for hardware and software, before ongoing licensing, maintenance, integration, and internal staff time are considered.
That timeline matters for staff safety. RTLS projects often involve readers, cabling, network planning, zone configuration, integrations, testing, and training. For asset tracking, a phased rollout may be acceptable. For workplace violence response, waiting months for full coverage can leave frontline staff exposed.
Privacy and Staff Adoption
A staff safety badge only works if staff actually wear it. Continuous location tracking can raise privacy concerns, especially in clinical and behavioral health environments where teams may worry about being monitored during breaks, room visits, charting time, or movement across units.
That does not mean RTLS cannot work. It means adoption has to be treated as part of the safety plan. Non-tracking wearable duress systems reduce that barrier because they are built around alert-triggered location sharing, not continuous staff monitoring.
Compliance Does Not Require RTLS
The Joint Commission’s workplace violence prevention read focus on program structure, not one required technology. Hospitals need leadership oversight, staff training, reporting processes, data analysis, worksite analysis, response planning, and governing body accountability.
That gives hospitals flexibility. RTLS can support a workplace violence prevention program, but it is not the only path. A dedicated staff duress system, paired with clear policies, training, response workflows, incident reporting, and leadership review, can support the same prevention and response goals without full continuous location-tracking infrastructure.
What Are the Real Alternatives to RTLS for Hospital Staff Safety?
The term “RTLS alternatives” is still relatively new in the healthcare safety conversation. For years, hospitals were often presented with RTLS as the default infrastructure investment for staff safety. But staff protection doesn’t always require continuous tracking. The actual landscape of non-tracking staff safety technology is broader, and in many cases, more practical than that framing suggests.
For hospitals evaluating their options, the right question is not only, “Can this system locate someone?” The better question is, “Can staff call for help quickly, can responders understand where to go, and can the system be adopted without creating privacy concerns?” This guide to healthcare panic button systems walks through the main options in more detail.
Wearable Non-Tracking Panic Button Systems
The most direct replacement for RTLS in a staff safety context is a wearable duress badge that activates only when pressed. The badge remains silent and private during normal operations. When a staff member feels threatened, a single button press transmits an alert to responders. Approximate location can be determined through system design, nearby infrastructure, or defined zones, giving the response team enough context to act without continuous location logging.
This event-triggered model has a practical adoption advantage. Staff are more likely to trust a badge that is designed for emergency activation, not routine monitoring. A badge that gets worn consistently, and is supervised to confirm it remains active and connected, is far more valuable than a tracking badge that staff avoid, remove, or leave behind because they are uncomfortable with continuous visibility.
BERT Team and Nurse Call System Integration
Behavioral Emergency Response Teams, or BERT teams, represent the operational layer that makes staff safety technology work. The technology sends the alert, but the response workflow determines who receives it, who responds, and how the incident is managed.
For hospitals that already have nurse call infrastructure, adding portable staff duress pendants or staff assist features may be a lower-cost path than a full RTLS deployment. This approach can work well when the facility has reliable coverage, clear escalation procedures, and trained response teams.
Two-Way Radios With Dedicated Duress Function
Many hospitals already use two-way radio infrastructure for security, facilities, transport, and operational coordination. Modern radio platforms can include dedicated one-touch duress buttons that transmit an emergency alert to a dispatch center or security team.
This option is most practical for teams that already carry radios as part of their daily workflow. For hospitals with existing radio coverage, enabling the duress function may require less new infrastructure than RTLS. The limitation is coverage consistency, since most clinical staff do not carry two-way radios throughout every shift.
Fixed Panic Stations at High-Risk Locations
Fixed panic buttons can be installed in areas with predictable risk, such as registration desks, triage areas, psychiatric intake rooms, emergency department check-in, and reception points. OSHA notes that hospital staff with direct patient contact are at higher risk of workplace violence, especially in emotionally charged situations involving fear, lack of control, weapons, drugs, alcohol, or violence.
Fixed panic stations do not provide full mobile staff coverage, but they can still address important risk zones. They are best viewed as part of a layered safety plan, especially when paired with wearable devices or a defined response workflow.
How Do Non-Tracking Panic Button Systems Actually Work?
Non-tracking systems are simpler in design than RTLS, and that simplicity is their main operational advantage. When a staff member feels threatened, they press a discreet button on a wearable badge or lanyard. Pinpoint panic button systems also support two button options: one for de-escalation and one for panic, which helps reduce accidental alerts while still giving staff a fast way to call for help.
The badge transmits an alert signal to receivers distributed throughout the facility. The alert is then routed to the right response point, such as security, a nurse station, a central monitoring team, or a designated response workflow. Most systems include the staff member’s identity, badge ID, and approximate location, such as room, zone, or nearest receiver.
What does not happen is just as important. The badge does not continuously broadcast staff location during normal operations. There is no routine movement trail showing where a nurse was throughout the shift, and no supervisor dashboard built around real-time staff tracking. A supervised system can still confirm that devices are active and connected, without turning the badge into a continuous tracking tool.
Response speed depends on coverage, alert routing, and the hospital’s internal response process. But for staff safety, the value is straightforward: staff can trigger help discreetly, responders receive usable location context, and the system supports privacy because it activates only when help is requested.
How Should Hospitals Compare RTLS and Non-Tracking Duress Systems?
It is whether the system matches the safety outcome the hospital needs. RTLS for staff safety is built around continuous location visibility across rooms, corridors, assets, patients, and staff. That broader scope can be valuable when the hospital also needs asset tracking, patient flow visibility, or operational location data.
Non-tracking duress systems are scoped differently. They focus on staff panic buttons, alert routing, receiver coverage, badge supervision, and emergency response workflows. For hospitals that mainly need workplace violence response, the question is whether full RTLS infrastructure is necessary, or whether a focused staff duress system can deliver the response outcome more directly.
RTLS vs. RTLS Alterntaives Duress System: Side-by-Side Comparison
| Factor | Full RTLS System | Non-Tracking Duress System |
|---|---|---|
| Tracking model | Continuous location visibility | Alert-triggered location context |
| Primary safety use case | Asset, patient, and staff tracking | Staff duress alerting and emergency response |
| Staff privacy concern | Higher, continuous staff visibility | Lower, activates only when help is requested |
| Badge wear compliance | Variable, especially if staff perceive surveillance risk | Easier to support because the device is not used for routine monitoring |
| IT infrastructure required | Higher, readers, servers, integrations, network planning | Lower, focused on badges, receivers, supervision, and alert routing |
| Deployment planning | More complex when room-level or facility-wide coverage is required | Depends on layout, receiver count, cabling needs, and alert-routing setup |
| Deployment Timeline | Typically 3 to 12 months depending on facility size, integrations, and change management | Typically 4 to 12 weeks with minimal infrastructure changes required |
| Maintenance model | Broader system maintenance, software, integrations, and infrastructure support | Device supervision, maintenance plan, portal access, and alert license requirements |
| Joint Commission workplace violence support | Yes, when paired with policies, training, reporting, and response workflows | Yes, when paired with policies, training, reporting, and response workflows |
| Best fit | Hospitals needing broad operational location visibility | Hospitals prioritizing staff safety, privacy, and rapid duress response |
| Behavioral health fit | Mixed, privacy concerns may affect adoption | Strong, especially where staff trust and privacy matter |
The comparison becomes clearer when adoption is part of the decision. A broad location platform may be useful for operational visibility, but staff safety depends on whether workers carry the device, trust the system, and activate it during a real incident.
Which Healthcare Settings Benefit Most from Non-Tracking Systems?
Non-tracking duress systems are strongest in healthcare settings where staff move frequently, risk can escalate quickly, and continuous tracking may create adoption concerns. They are not the right answer for every clinical scenario, but they are a strong fit when the priority is discreet alerting, supervised wearable protection, and fast response.
Behavioral Health and Psychiatric Units
Behavioral health is one of the strongest use cases for non-tracking panic buttons. Staff often work in close proximity to patients during high-acuity or unpredictable situations, and the alert needs to follow the staff member, not just the room.
BLS data shows how severe the risk can be in this environment. Psychiatric aides experienced a workplace violence DART rate of 543.6 cases per 10,000 full-time workers in 2021/2022, one of the clearest indicators that behavioral health teams need practical, wearable staff protection.
For these units, a non-tracking system fits the workflow because it gives staff a discreet way to call for help, while avoiding continuous location monitoring during normal care.
Small and Community Hospitals
Small and community hospitals often need staff safety coverage without taking on a large infrastructure project. A non-tracking duress system can be easier to scope because it focuses on wearable badges, receiver coverage, supervision, and alert routing instead of full RTLS deployment across every room and corridor.
This makes it a practical option for facilities that want to improve hospital staff safety quickly, especially when the immediate need is emergency response rather than asset tracking or patient flow visibility.
Residential Rehabilitation Facilities
Residential rehab facilities face safety risks from behavioral escalation, co-occurring mental health conditions, substance-related incidents, and lower staffing density. These facilities often need a staff safety system that works reliably without heavy IT involvement.
A wearable, non-tracking model is a strong fit because it gives staff mobile protection across bedrooms, common areas, therapy rooms, intake areas, and outdoor spaces where fixed panic buttons may not be enough.
Emergency Departments
Emergency departments are a mixed-fit environment. Risk is high, but workflows are more complex. Triage, registration, waiting rooms, and treatment areas may each need a different layer of protection.
For EDs, the best approach is often layered: fixed panic buttons in predictable high-risk points, plus wearable panic buttons for mobile staff. This gives hospitals broader coverage without requiring full RTLS for staff safety as the first step.
See How Pinpoint Works as an RTLS Alternative for Staff Safety
If your priority is staff duress response, not continuous location tracking, Pinpoint gives healthcare teams a focused alternative to full RTLS infrastructure.
Pinpoint’s non-tracking, supervised wearable panic button system is designed for behavioral health, acute care, and other high-risk healthcare environments. Staff can activate help quickly, responders receive actionable location context, and the system supports privacy by avoiding continuous staff tracking during normal shifts.
FAQ’s
Do non-tracking staff safety systems meet Joint Commission NPG.02.04.01 requirements?
Yes. Joint Commission standard NPG.02.04.01, effective January 2026, requires hospitals to have a formal workplace violence prevention program with trained leadership, annual risk assessments, and governing body reporting, but does not mandate RTLS technology. A non-tracking wearable duress system, paired with BERT team protocols, documented training, and incident reporting, meets all NPG.02.04.01 program requirements
What is the best alternative to RTLS for hospital staff safety?
The best alternative is a non-tracking wearable duress system. Staff wear a discreet panic button that activates only when pressed, collecting no location data during normal shifts. When triggered, the alert includes approximate location, badge ID, and responder routing. These systems cost less than RTLS, deploy faster in 30 to 90 days, and raise fewer privacy concerns because staff are not continuously tracked.
What types of duress systems can hospitals use instead of RTLS?
Hospitals can use wearable panic buttons, supervised duress badges, nurse call integrations, BERT team activation workflows, two-way radios with duress buttons, and fixed panic stations. The right option depends on staff mobility, facility layout, risk areas, response workflow, and whether privacy-conscious alerting is a priority.
Is a non-tracking duress system cheaper than RTLS?
In many cases, yes. RTLS usually requires more infrastructure because it supports continuous location visibility across rooms, corridors, assets, patients, and staff. A non-tracking duress system is more focused on staff panic buttons, alert routing, supervision, and response workflows, which can reduce cost and deployment complexity.
How do non-tracking panic buttons protect staff privacy?
Non-tracking panic buttons protect privacy by staying inactive during normal work. They do not create a continuous movement trail or supervisor dashboard showing where staff are throughout the shift. Location context is shared only when the staff member activates an alert and needs help.
- How Serious Is the Hospital Workplace Violence Crisis?
- What Is RTLS and Why Are Hospitals Buying It for Staff Safety?
- Why Are Hospitals Reconsidering RTLS for Staff Safety?
- What Are the Real Alternatives to RTLS for Hospital Staff Safety?
- How Do Non-Tracking Panic Button Systems Actually Work?
- How Should Hospitals Compare RTLS and Non-Tracking Duress Systems?
- Which Healthcare Settings Benefit Most from Non-Tracking Systems?
- See How Pinpoint Works as an RTLS Alternative for Staff Safety
- FAQ’s
Author:
Jordan Belous
Chief Marketing Officer of Pinpoint North America, where she leads marketing strategy, brand development, and digital growth initiatives. She earned a Bachelor of Science in Allied Health with a concentration in physical therapy sciences from the University of Tampa, bringing a unique interdisciplinary perspective that blends healthcare knowledge with modern marketing strategy.
Jordan writes about workplace violence prevention in healthcare, nurse safety, staff wellbeing, and emerging healthcare technologies that support frontline teams. Her work explores how hospitals and behavioral health facilities can build safer environments, reduce burnout and turnover, and implement safety systems that protect staff while preserving trust and dignity.
She is also the Chief Executive Officer of Whip Pediatric Cancer, a nonprofit dedicated to supporting children battling cancer and raising awareness and funds for pediatric cancer. Through her work with Whip, Jordan regularly visits pediatric cancer patients in hospitals and spends time alongside patients, families, and the clinicians who care for them. These experiences place her directly beside nurses and healthcare teams every day and reinforce her belief that the people providing care deserve to feel just as safe as the patients they serve.
Her experiences with Whip and her work at Pinpoint are closely connected, both driven by her deep respect for nurses and frontline healthcare workers. Seeing firsthand the compassion, resilience, and critical role nurses play has strengthened her commitment to advocating for safer healthcare environments and ensuring that those who dedicate their lives to caring for others have the protection and support they deserve.