
Duress Alert Solutions for Healthcare: Wearable vs. Fixed Systems

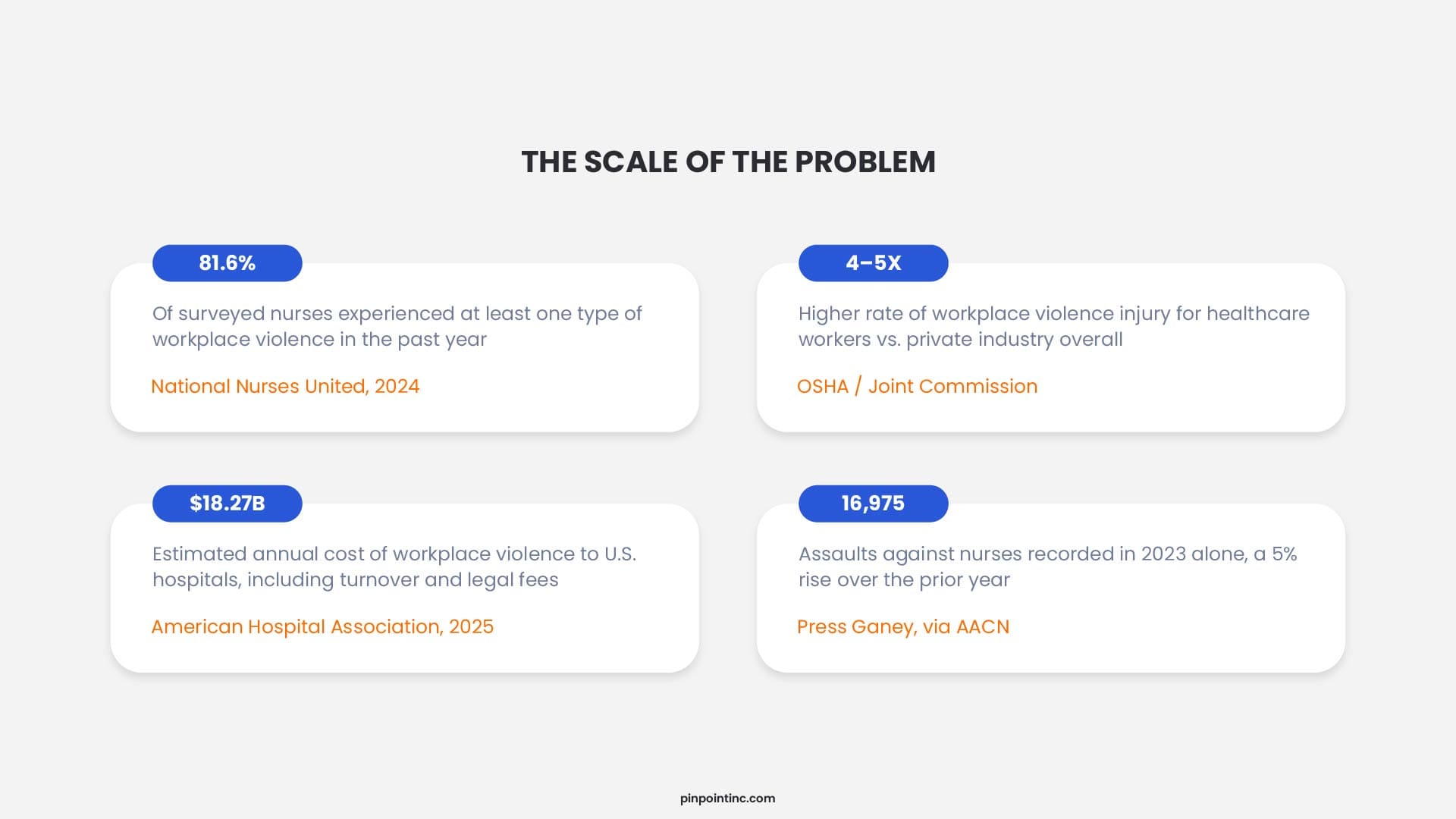
Here’s a number worth sitting with for a second: 81.6 percent. That’s the share of nurses who told National Nurses United in 2024 that they had experienced at least one type of workplace violence in the previous year, everything from verbal threats to physical assault. Now here’s the part that doesn’t quite add up. In a large share of the hospitals where those nurses work, the primary tool for calling for help is still bolted to a wall.
Healthcare workers face violence at roughly four to five times the rate of the average private-sector employee, a figure the Occupational Safety and Health Administration has tracked for years and the Joint Commission now cites directly in its safety guidance. The American Hospital Association’s 2025 Burden of Violence report put the annual cost of this violence to U.S. hospitals at roughly $18.27 billion once turnover, workers’ compensation, legal fees, and care for injured staff are added together.
Every one of those statistics traces back to the same unglamorous, practical question: when something goes wrong, how does a caregiver actually call for help, and how long does that call take to reach someone who can act on it? That question is the entire reason a duress alert solution exists in the first place, and it’s also why the choice between a wearable system and a fixed system is not a minor procurement detail. It decides whether protection follows the caregiver through the building, or waits patiently for the caregiver to find it.
What a Duress Alert Solution Actually Has to Do
Strip away the marketing language and a wearable duress alert solution has exactly three jobs. It needs to let a staff member signal distress, silently or audibly, without requiring complicated steps in a moment when fine motor control and clear thinking are both in short supply. It needs to transmit that signal to the right responders immediately, not after a delay for human dispatch to interpret it. And it needs to tell those responders where to go, ideally down to the room or bed, not just the floor or the wing.
That third job is where a lot of older infrastructure quietly fails. An alert that says someone needs help but can’t say where it loses most of its value the moment a corridor has more than a couple of doors on it.
It’s worth pausing on one related distinction here too, because buyers often blur it. Not every alert is supposed to look the same. A loud, visible panic alarm is built to interrupt a dangerous situation immediately, while a quieter duress signal is designed for moments when drawing attention could make things worse, and that difference matters more than most buyers realize once they actually start comparing systems side by side.
Two Architectures, One Underlying Decision
Most duress technology on the market today is built on one of two physical architectures. A wearable system rides with the caregiver, usually as a badge, clip, or wristband that stays on the body through every room change, hallway, and parking lot crossing. A fixed system stays exactly where it’s installed, typically a button under a reception desk, inside a medication room, or mounted near a nurses’ station.
There’s a broader taxonomy of healthcare panic button types worth knowing about too, including mobile apps and real-time locating platforms, each with its own trade-offs around accuracy, battery life, and IT dependency. That’s a deeper conversation on its own. For this comparison, wearable and fixed are the two architectures that actually determine almost every practical safety decision a hospital makes, so that’s where we’ll spend most of our time.
Wearable Duress Systems: Protection That Travels With the Caregiver
A wearable duress device is built around one assumption: danger doesn’t politely wait for staff to be near a fixed point, so the safety tool shouldn’t depend on one either. Most designs today take the form of a badge worn on a lanyard or reel, sitting right alongside a staff ID, which means it requires no new habit beyond what nurses already do every shift.
The advantage is straightforward. Whether a caregiver is inside a patient’s bathroom, a supply closet, an elevator, or the far end of a behavioral health unit, the device is already there. When it’s pressed, the alert and the caregiver’s location at that moment travel together, so responders aren’t searching a building, they’re walking directly to a room. Adoption already reflects this shift; Campus Safety’s 2024 survey of hospitals found that 68 percent already issue mobile panic buttons on pendants to staff.
The trade-offs are mostly operational rather than functional. Devices need to be charged, which means facilities need a charging and replacement routine that doesn’t quietly fall apart on a busy week. Cost per unit is generally higher than a single fixed button, since every staff member who needs coverage needs their own device. And adoption matters more than people expect going in. A wearable badge that staff find uncomfortable, confusing, or easy to forget at the start of a shift provides exactly zero protection no matter how well it was engineered.
The systems gaining the most traction tend to be the ones built like a standard wearable panic button designed to sit quietly on a badge until the moment it’s actually needed, rather than something staff have to consciously remember to use.
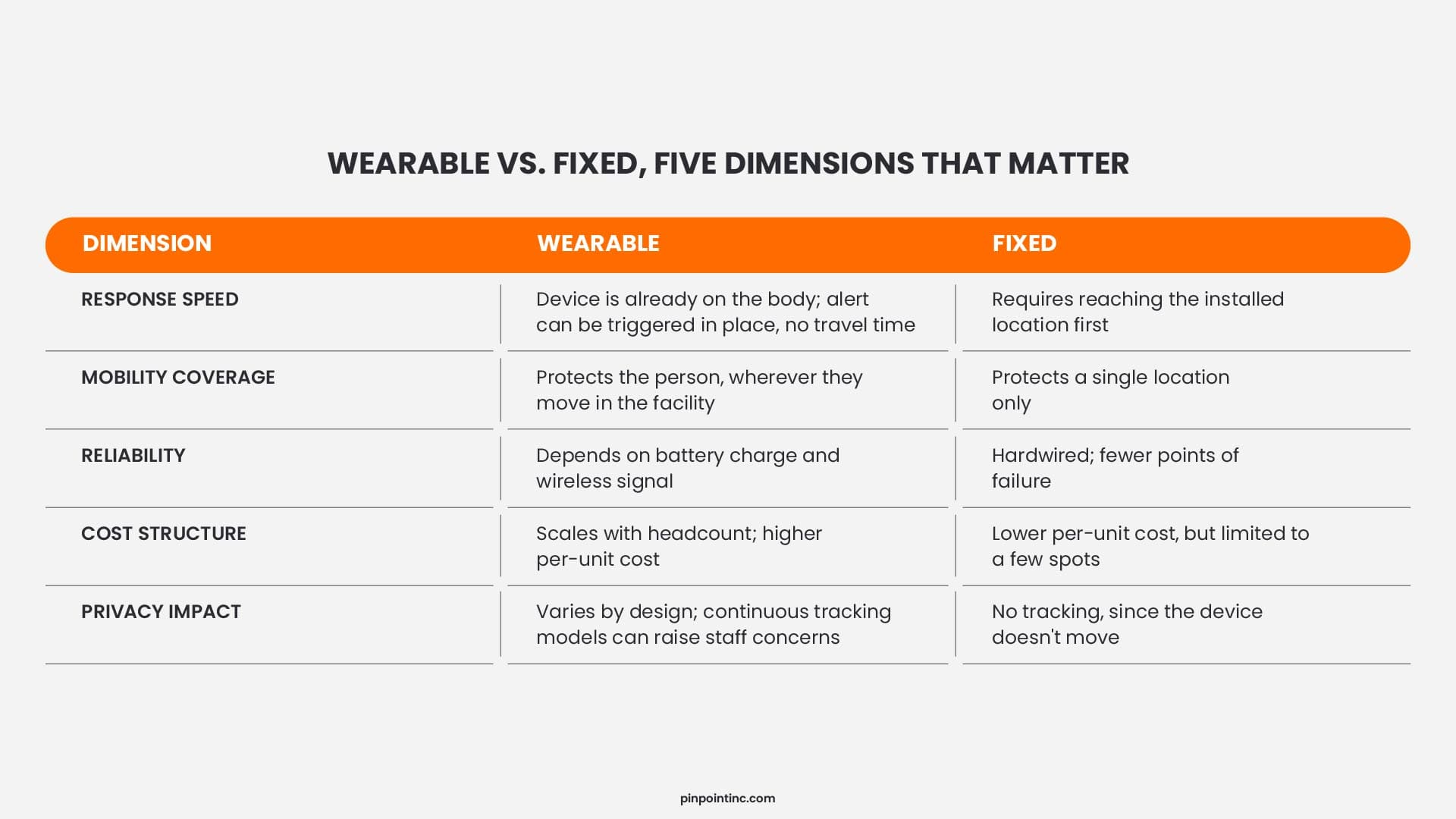
Fixed vs. Wearable Duress System: The Mobility Gap That Changes Everything
Fixed systems have one major strength: they’re hard to break. A hardwired button under a reception desk or beside a medication cabinet doesn’t need charging, doesn’t lose signal, and doesn’t depend on a staff member remembering to wear anything. For roles that genuinely stay at one station for most of a shift, a fixed device covering that exact spot is inexpensive, reliable, and easy to justify on a budget line.
The limitation is just as simple, and it’s the one that matters most in an actual emergency. A fixed button only works if the person needing help can physically reach it. In a real assault, that’s often the first thing that’s no longer true. Caregivers describe being cornered, pinned, or pulled away from the very point where the button lives, and that gap between “help exists somewhere in the building” and “help is reachable right now” is exactly where fixed-only systems tend to fail when it counts.
That gap matters even more now that risk doesn’t sit still the way it used to. Real-world duress alert data shows that incidents have spread out fairly evenly across all seven days of the week, with alerts clustering around midday and the late-afternoon shift change rather than a handful of predictable high-risk days. When danger can show up almost anywhere, at almost any hour, a tool that only works in one fixed spot is solving half the problem. A wearable non-RTLS system, by contrast, travels with the caregiver and ensures that protection is always within reach, no matter where or when an incident occurs. That mobility is what transforms a duress alert solution from a static safety measure into a dynamic layer of protection that actively follows staff through every part of their shift.
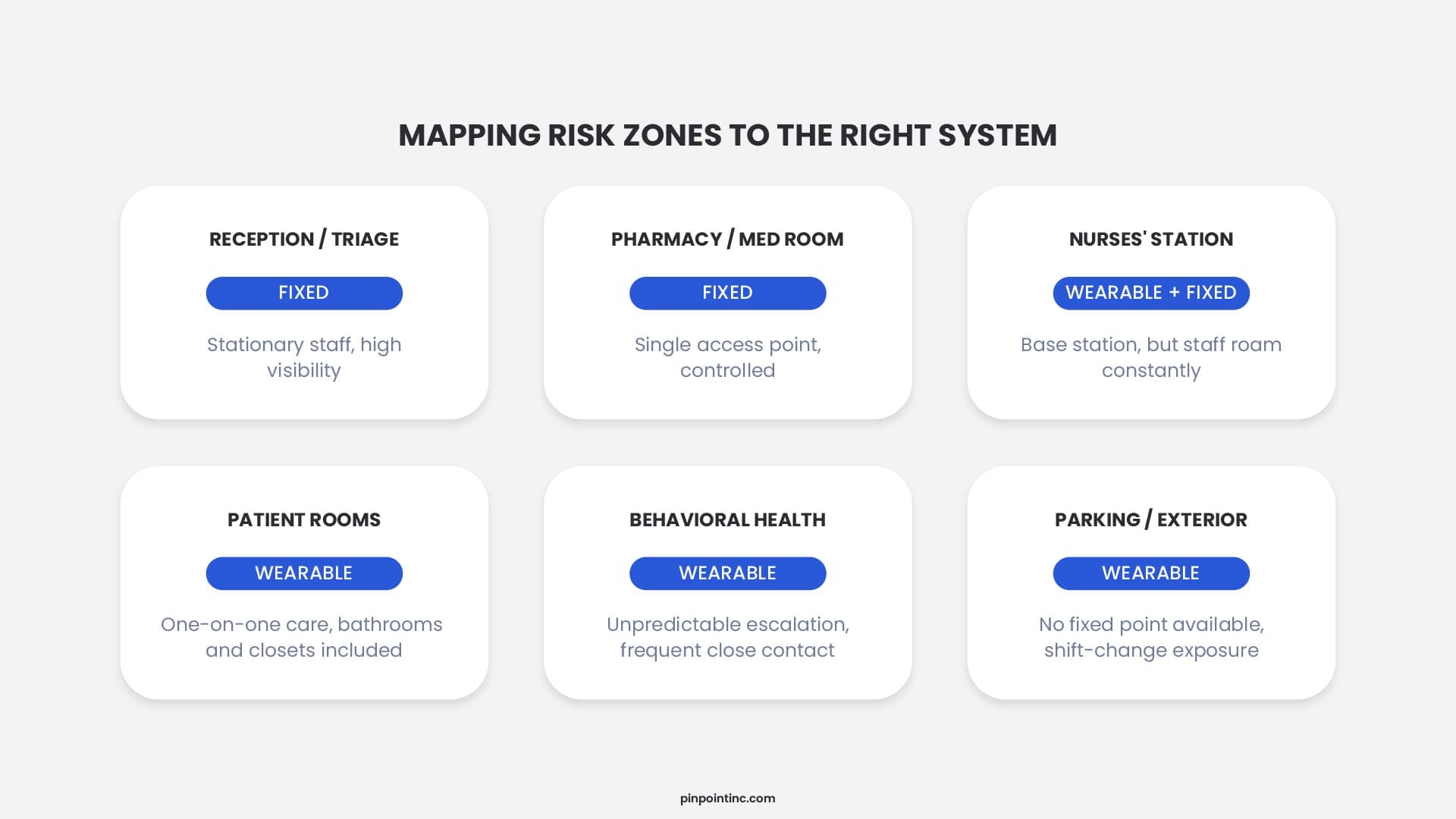
Where Each System Earns Its Place: Mapping Risk Zones to the Right Solution
In practice, almost no hospital makes a single, binary choice between the two. The more useful exercise is mapping risk by zone rather than picking a winner. A reception desk, a triage window, or a pharmacy counter, all places where one person sits in roughly the same spot for hours, are reasonable candidates for a fixed device as a dependable, low-maintenance backup. Patient rooms, behavioral health units, parking structures, and anywhere staff move between locations all shift are squarely wearable territory, since that’s exactly where a fixed button can’t follow.
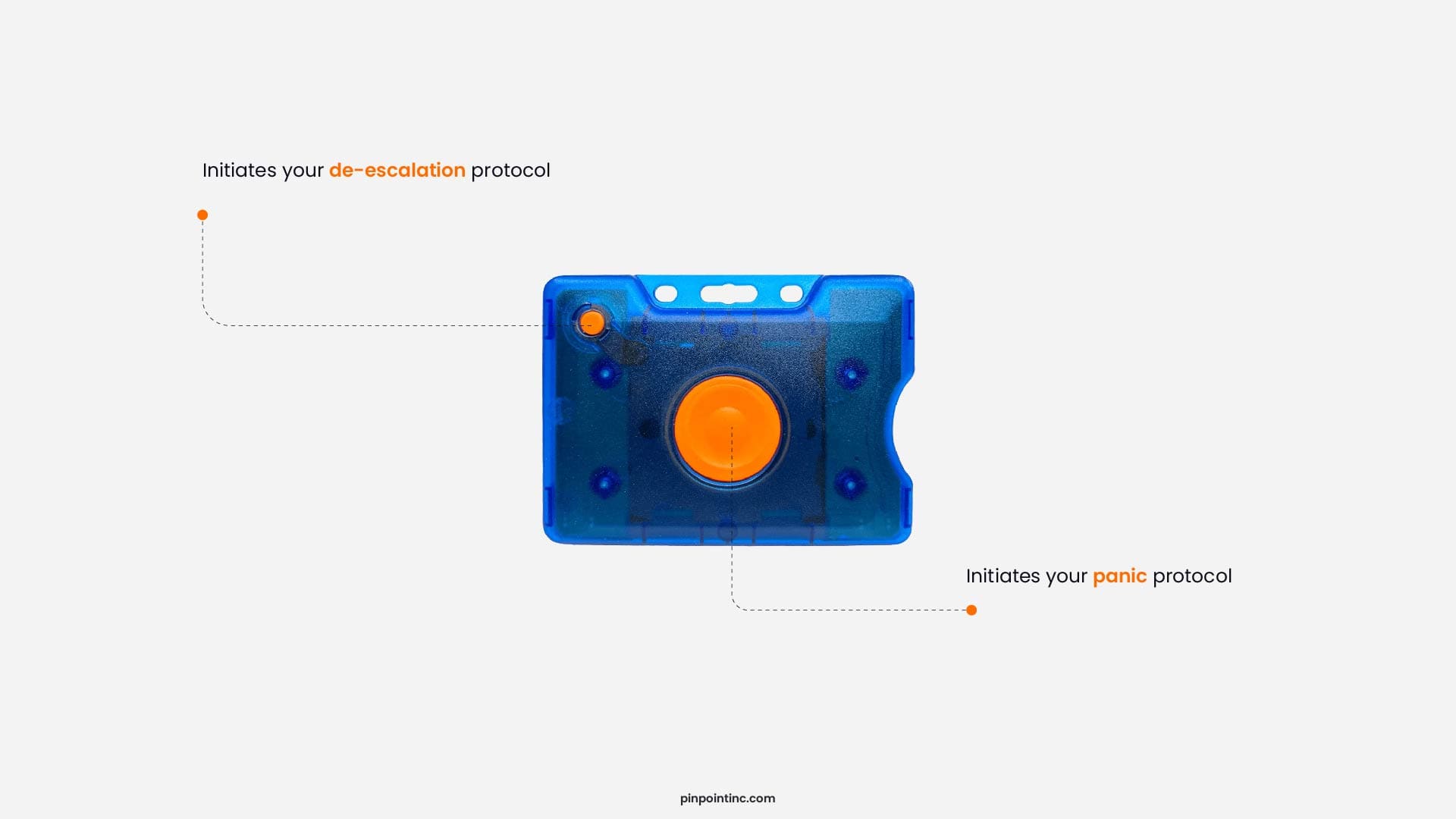
It’s also worth understanding the distinction between de-escalation and panic alerts, since the two serve fundamentally different purposes . A de-escalation alert is used when a situation begins to escalate but hasn’t yet become an emergency, such as when a patient becomes verbally aggressive, starts pacing, or shows early signs of agitation . This alert is discreet and silent, designed to bring nearby support before the situation spirals, allowing staff to intervene early without drawing attention that could make things worse . A panic alert, by contrast, is meant for immediate threats where physical harm is imminent or already occurring . It triggers an urgent, often audible response, signaling that help is needed right now . Many modern systems, including Pinpoint’s platform, offer both options within a single wearable device, so staff can choose the right response for the moment without needing to reach a fixed point .
General hospital settings tend to need both layers working together because the risk itself isn’t uniform across the building. An emergency department waiting area behaves nothing like a labor and delivery floor, which behaves nothing like an underground parking garage at the end of a night shift. Mapping out where staff actually spend unsupervised one-on-one time with patients or the public, then matching that map against which system actually reaches which zones, turns a vague safety initiative into a specific coverage plan that a facilities or security director can defend in a budget meeting.
Why Response Time Is the Number That Actually Matters
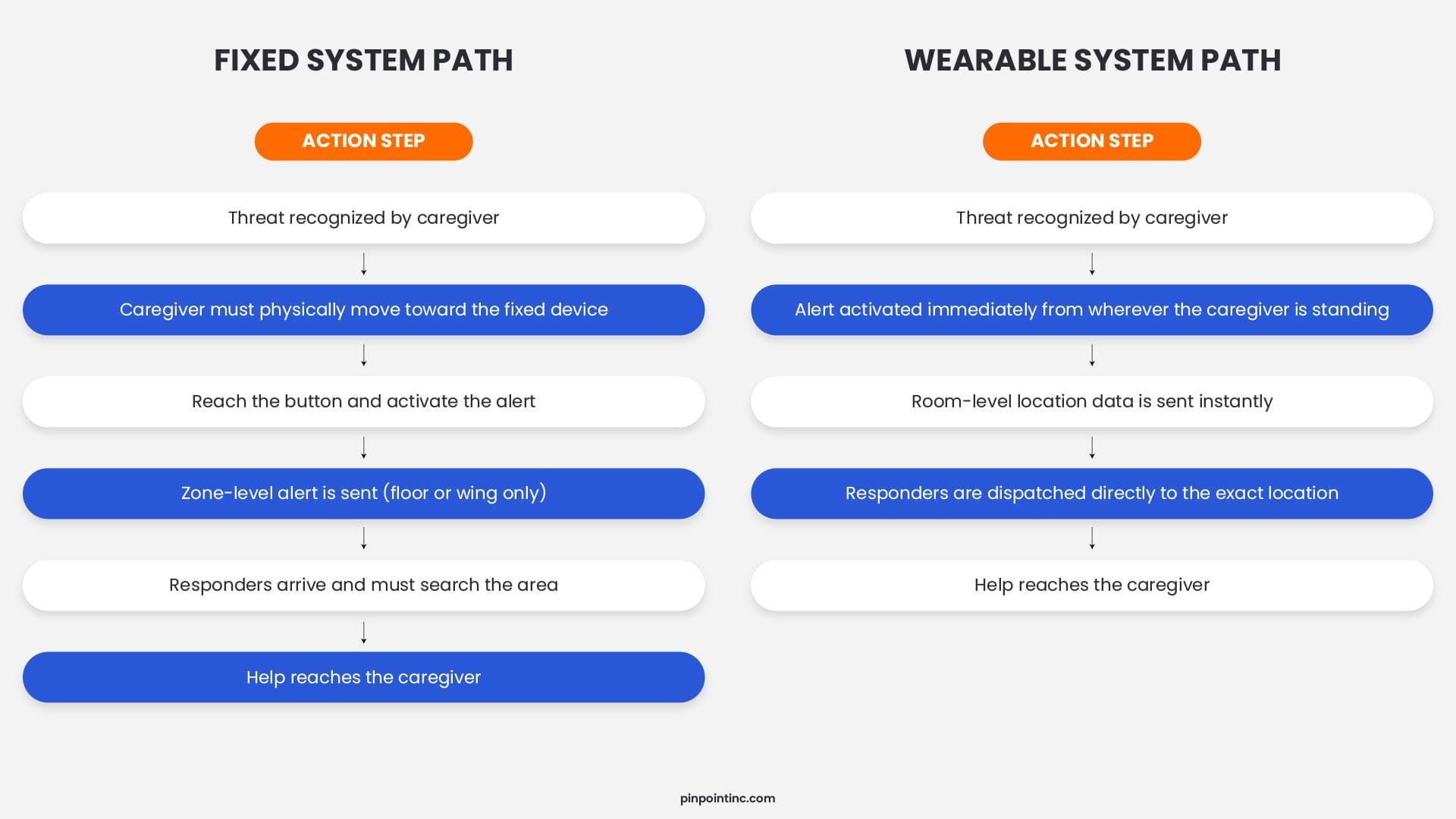
It’s tempting to evaluate duress technology by feature checklist, but almost everything on that checklist exists in service of one number: how many seconds pass between a threat starting and help physically arriving. Every additional step in that chain, unlocking a phone, walking toward a wall, waiting for a dispatcher to interpret a vague alert, adds time that a hospital generally doesn’t have during an active incident.
A fixed system’s time to help is, by definition, the time it takes to physically reach the button plus the time it takes responders to arrive. A wearable system removes that first variable almost entirely, since the device travels with the person and most modern designs trigger an alert with a single press from wherever the caregiver happens to be standing. The remaining variable, how precisely the system can tell responders where to go, is where location accuracy earns its keep. A general alert that only narrows a search down to “third floor” still costs precious time compared to one that resolves straight to a specific room or bed.
Compliance Pressure Is Building Around This Decision
This isn’t purely an operational question anymore either. The Joint Commission’s workplace violence prevention standards have been in effect for hospitals and critical access hospitals since January 2022, and the agency expanded similar requirements to behavioral health and human services organizations in mid-2024, then to assisted living communities, nursing care centers, and office-based surgery practices in mid-2025. Those standards require a documented prevention program, regular risk assessments, incident reporting, and ongoing staff training. None of it mandates a specific brand of duress device, but all of it is far easier to demonstrate during a survey with a system that actually generates location and response-time data rather than a paper policy and good intentions.
Explore our resources for more practical guides on staff safety, compliance, and duress technology.
OSHA has leaned on its General Duty Clause to cite facilities that fail to address known violence risks, and federal appellate courts have begun upholding those citations against healthcare organizations, which raises the practical stakes well beyond a single bad incident report. None of this means every facility needs to rip out its existing infrastructure overnight. It does mean that when hospitals sit down to compare options for the year ahead, including the side-by-side vendor research many facilities now run before locking in next year’s panic button vendor, compliance documentation and response analytics are increasingly part of the scorecard, not an afterthought. Many facilities also find it useful to start from a complete reference architecture that maps detection, notification, and response into a single system before they get as far as comparing vendors at all.
A Practical Framework for Choosing the Right Duress Alert Solution
Boiled down, the decision usually rests on five questions worth asking before anyone signs a contract.
- How much do staff actually move during a shift, and where do they go?
If staff spend most of their time at a single workstation, a fixed device might be sufficient. But if they’re constantly moving between patient rooms, hallways, stairwells, and parking structures, a wearable system is non-negotiable. Walk a shift with your team and map their actual movement patterns. You’ll likely discover staff cover far more ground than you realized, and that’s exactly where a fixed device can’t protect them.
- How dependent is the proposed system on hospital Wi-Fi, network uptime, and ongoing IT support?
Systems that rely heavily on hospital Wi-Fi introduce a critical vulnerability. If the network goes down, so does your duress alert system. Look for solutions that operate independently of Wi-Fi or have robust backup protocols. Also consider the IT burden. Some systems require ongoing network maintenance, firmware updates, and dedicated IT support, which adds hidden costs and complexity. The most reliable solutions work when you need them most, regardless of network conditions.
- What does the full cost look like over five years, not just the installation invoice?
The sticker price is only the beginning. Factor in ongoing licensing fees, maintenance contracts, battery replacements, IT support hours, and potential network upgrades. A system that appears cheaper upfront can end up costing significantly more over time. Ask vendors for a detailed five-year cost projection, including all recurring expenses, so you can make an apples-to-apples comparison.
- Will staff actually wear or use it consistently, or will it end up in a drawer by week two?
Adoption is the single most overlooked factor. A beautifully engineered device provides zero protection if staff find it uncomfortable or easy to forget. Look for badge-style devices that clip onto lanyards alongside staff IDs. Also consider privacy: non-tracking wearable systems that only activate location data when the button is pressed are generally more trusted by staff than systems that monitor location continuously. When staff know their movements aren’t being tracked all day, they’re far more likely to wear the device consistently.
- Does it generate the kind of incident and response-time data that supports both compliance reporting and internal safety reviews?
The Joint Commission requires documented prevention programs, incident reporting, and ongoing risk assessments. OSHA enforcement actions increasingly depend on demonstrated hazard controls. A duress system that generates detailed incident logs, response-time analytics, and location data transforms a safety investment into a compliance asset. Without this data, you’re left with anecdotal evidence and paper policies, both difficult to defend during a survey or citation review.
CTA: For a deeper dive into real-world applications, explore our complete resource library for more insightful guides.
See It In Context
Spec sheets make every duress alert solution sound roughly the same. The trade-offs between wearable and fixed coverage become obvious only once you see a system respond to your actual floor plan, shift patterns, and existing network. That’s exactly what a live demo shows, walking through how a layered wearable-and-fixed approach behaves inside your facility.
Pinpoint was built to meet every requirement that matters. Need a non-tracking wearable that respects staff privacy? Yes. Looking for compliance-ready incident and response-time data? Built in. Want a device staff actually wear shift after shift? Our badge-style wearables integrate seamlessly into existing workflows. Operating independently of hospital Wi-Fi means you’re never vulnerable during network outages or cyber threat. Two alert options, discreet de-escalation and urgent panic, all from a single device. We designed Pinpoint to protect your people without complicating their day.
Schedule a Demo and see how Pinpoint fits your facility.
See Pinpoint in Action
Request a live demo to see how Pinpoint performs in your clinical environment.
2026 Key Insight
The dominant deployment pattern in 2026 is tiered coverage. Hospitals are placing IR in emergency departments, behavioral health units, and inpatient wings where precision is life critical. They are using BLE in lobbies, parking structures, and administrative areas where near-room accuracy is sufficient and cost matters more.
Industry Insight
RTLS systems in healthcare are effective for tracking and operational visibility, but their real-world success depends heavily on change management, system complexity, and staff adoption – Source
FAQ’s
What is a duress alert solution in healthcare?
A duress alert solution is a system that lets healthcare staff signal for help during a threatening or dangerous situation and automatically routes that alert, along with location information, to security or another designated responder. It can be silent or audible, and it can be built on a wearable, fixed, mobile-app, or real-time-locating architecture depending on the environment it’s protecting.
What's the main difference between a wearable and a fixed duress alert system?
A wearable system travels with the staff member as a badge, clip, or wristband, so it works wherever they go during a shift. A fixed system stays installed at one location, such as a reception desk or medication room, and only protects staff while they’re physically near it.
Can a hospital use both wearable and fixed duress systems together?
Yes, and most well-designed safety programs do exactly this. Fixed devices make sense at stationary, high-traffic points like front desks or pharmacy windows, while wearable devices cover staff who move between patient rooms, units, and outdoor areas throughout a shift.
Do healthcare facilities have to comply with specific workplace violence standards?
Hospitals accredited by the Joint Commission have been required to maintain a documented workplace violence prevention program since January 2022, and similar requirements now extend to behavioral health organizations, assisted living communities, nursing care centers, and office-based surgery practices. OSHA can separately cite facilities under its General Duty Clause for failing to address known violence risks.
Do wearable duress badges track staff location all day?
It depends on the vendor, and this varies more than buyers expect. Some platforms track location continuously throughout a shift, while others only determine location at the moment the button is actually pressed. Facilities concerned about staff privacy and day-to-day trust generally favor the second approach. Pinpoint’s wearable operates the same way, location data is only captured when a staff member activates an alert, so there’s no passive tracking or surveillance throughout the shift.
- What a Duress Alert Solution Actually Has to Do
- Two Architectures, One Underlying Decision
- Wearable Duress Systems: Protection That Travels With the Caregiver
- Fixed vs. Wearable Duress System: The Mobility Gap That Changes Everything
- Where Each System Earns Its Place: Mapping Risk Zones to the Right Solution
- Why Response Time Is the Number That Actually Matters
- Compliance Pressure Is Building Around This Decision
- A Practical Framework for Choosing the Right Duress Alert Solution
- See It In Context
- FAQ’s